

Improving natural ventilation in hospital waiting and consulting rooms to reduce nosocomial tuberculosis transmission risk in a low resource setting
- PMID: 30683052
- PMCID: PMC6347752
- DOI: 10.1186/s12879-019-3717-9
Improving natural ventilation in hospital waiting and consulting rooms to reduce nosocomial tuberculosis transmission risk in a low resource setting
Abstract
Background: TB transmission in healthcare facilities is an important public health problem, especially in the often-overcrowded settings of HIV treatment scale-up. The problem is compounded by the emergence of drug resistant TB. Natural ventilation is a low-cost environmental control measure for TB infection control where climate permits that is suited to many different areas in healthcare facilities. There are no published data on the effect of simple structural modifications to existing hospital infrastructure to improve natural ventilation and reduce the risk of nosocomial TB transmission. The purpose of this study was to measure the effect of simple architectural modifications to existing hospital waiting and consulting rooms in a low resource setting on (a) improving natural ventilation and (b) reducing modelled TB transmission risk.
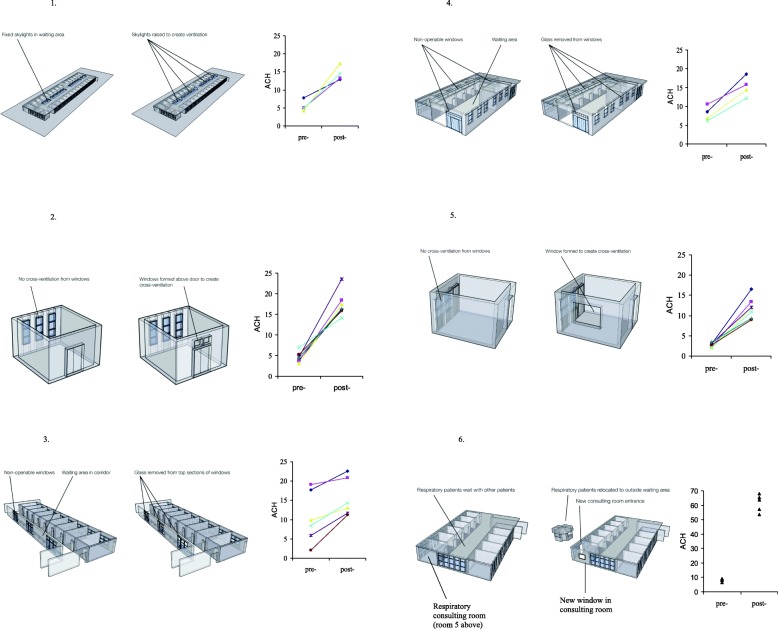
Methods: Room ventilation was measured pre- and post-modification using a carbon dioxide tracer-gas technique in four waiting rooms and two consulting rooms in two hospitals in Lima, Peru. Modifications included additional windows for cross-ventilation (n = 2 rooms); removing glass from unopenable windows (n = 2); creation of an open skylight (n = 1); re-building a waiting-room in the open air (n = 1). Changes in TB transmission risk for waiting patients, or healthcare workers in consulting rooms, were estimated using mathematical modelling.
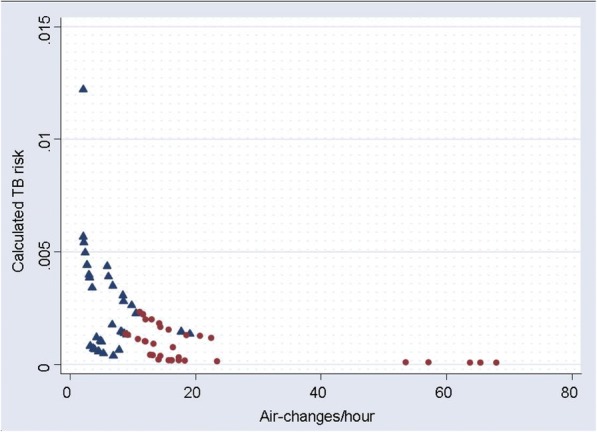
Results: As a result of the infrastructure modifications, room ventilation in the four waiting rooms increased from mean 5.5 to 15; 11 to 16; 10 to 17; and 9 to 66 air-changes/hour respectively; and in the two consulting rooms from mean 3.6 to 17; and 2.7 to 12 air-changes/hour respectively. There was a median 72% reduction (inter-quartile range 51-82%) in calculated TB transmission risk for healthcare workers or waiting patients. The modifications cost <US$75 in four rooms, and US$1000 and US$7000 in the remaining two rooms.
Conclusions: Simple modifications to existing hospital infrastructure considerably increased natural ventilation, and greatly reduced modelled TB transmission risk at little cost.
Keywords: Airborne transmission; Natural ventilation; Nosocomial transmission; Tuberculosis; Tuberculosis transmission; Waiting room.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was waived because the only human data related to average numbers of people in waiting rooms, or TB cases seen per day.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ewer K, Deeks J, Alvarez L, Bryant G, Waller S, Andersen P, Monk P, Lalvani A. Comparison of T-cell-based assay with tuberculin skin test for diagnosis of Mycobacterium tuberculosis infection in a school tuberculosis outbreak. Lancet. 2003;361(9364):1168–1173. doi: 10.1016/S0140-6736(03)12950-9. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
