

Contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the USA and Canada: a collaboration of cohort studies
- PMID: 30683625
- PMCID: PMC6589140
- DOI: 10.1016/S2352-3018(18)30295-9
Contributions of traditional and HIV-related risk factors on non-AIDS-defining cancer, myocardial infarction, and end-stage liver and renal diseases in adults with HIV in the USA and Canada: a collaboration of cohort studies
Erratum in
-
Correction to Lancet HIV 2018; 6: e93-104.Lancet HIV. 2019 Dec;6(12):e815. doi: 10.1016/S2352-3018(19)30106-7. Epub 2019 Apr 2. Lancet HIV. 2019. PMID: 30952566 No abstract available.
Abstract
Background: Adults with HIV have an increased burden of non-AIDS-defining cancers, myocardial infarction, end-stage liver disease, and end-stage renal disease. The objective of this study was to estimate the population attributable fractions (PAFs) of preventable or modifiable HIV-related and traditional risk factors for non-AIDS-defining cancers, myocardial infarction, end-stage liver disease, and end-stage renal disease outcomes.
Methods: We included participants receiving care in academic and community-based outpatient HIV clinical cohorts in the USA and Canada from Jan 1, 2000, to Dec 31, 2014, who contributed to the North American AIDS Cohort Collaboration on Research and Design and who had validated non-AIDS-defining cancers, myocardial infarction, end-stage liver disease, or end-stage renal disease outcomes. Traditional risk factors were tobacco smoking, hypertension, elevated total cholesterol, type 2 diabetes, renal impairment (stage 4 chronic kidney disease), and hepatitis C virus and hepatitis B virus infections. HIV-related risk factors were low CD4 count (<200 cells per μL), detectable plasma HIV RNA (>400 copies per mL), and history of a clinical AIDS diagnosis. PAFs and 95% CIs were estimated to quantify the proportion of outcomes that could be avoided if the risk factor was prevented.
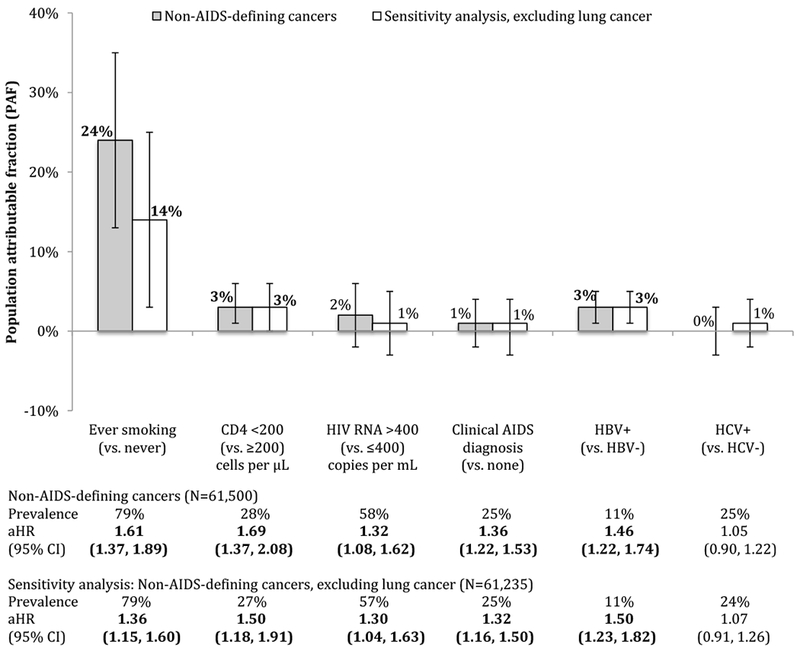
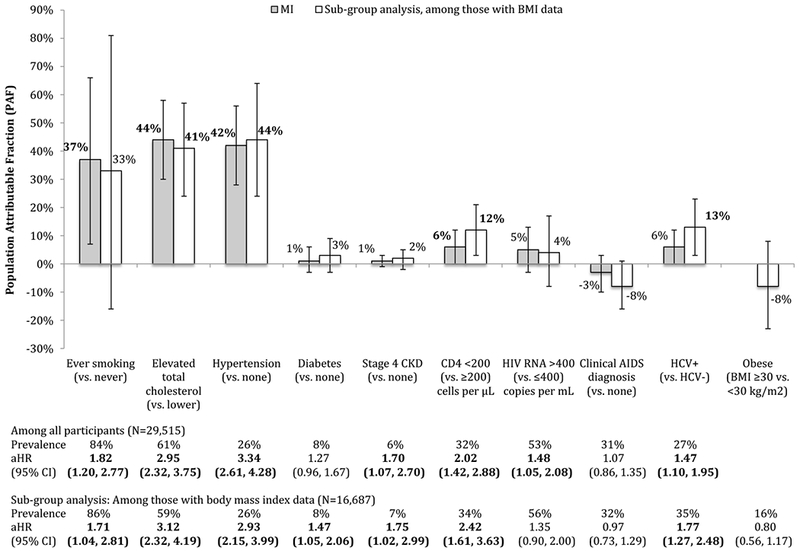
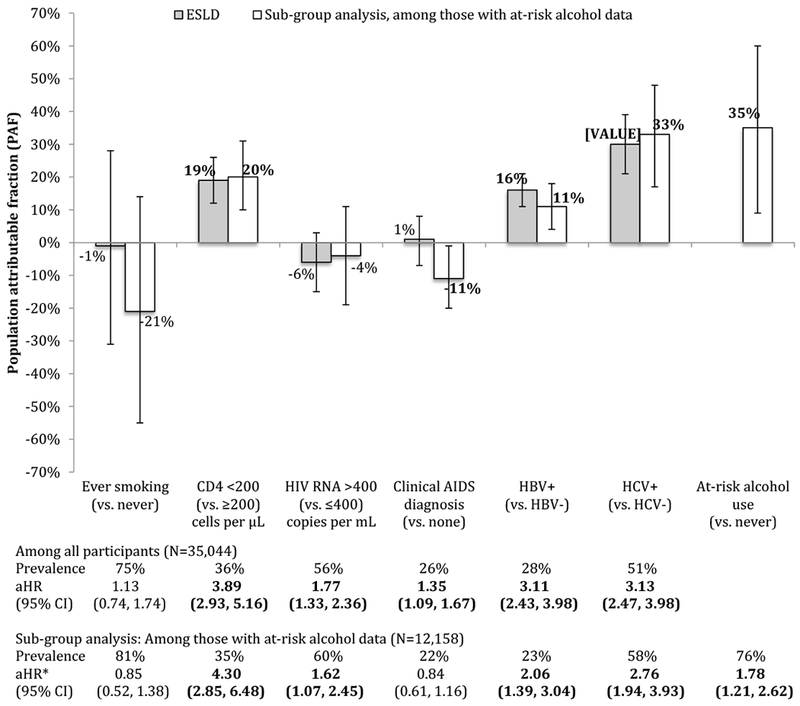
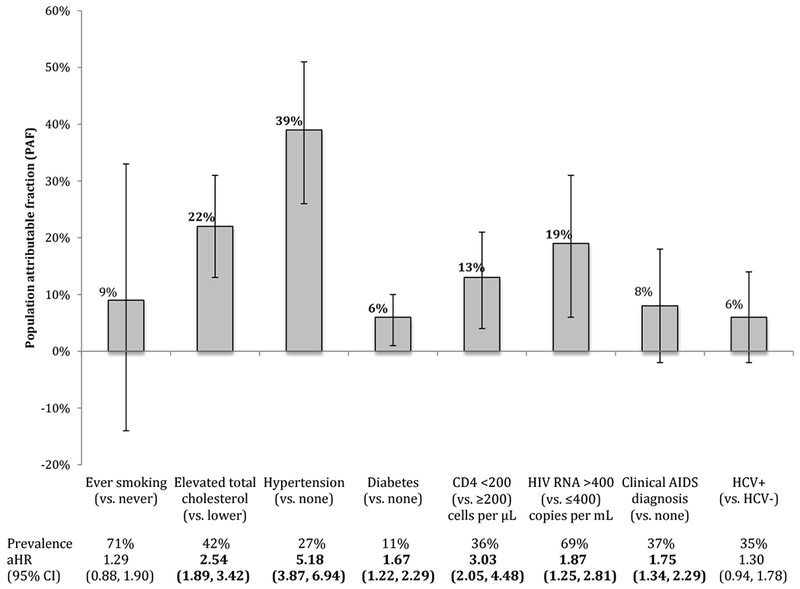
Findings: In each of the study populations for the four outcomes (1405 of 61 500 had non-AIDS-defining cancer, 347 of 29 515 had myocardial infarctions, 387 of 35 044 had end-stage liver disease events, and 255 of 35 620 had end-stage renal disease events), about 17% were older than 50 years at study entry, about 50% were non-white, and about 80% were men. Preventing smoking would avoid 24% (95% CI 13-35) of these cancers and 37% (7-66) of the myocardial infarctions. Preventing elevated total cholesterol and hypertension would avoid the greatest proportion of myocardial infarctions: 44% (30-58) for cholesterol and 42% (28-56) for hypertension. For liver disease, the PAF was greatest for hepatitis C infection (33%; 95% CI 17-48). For renal disease, the PAF was greatest for hypertension (39%; 26-51) followed by elevated total cholesterol (22%; 13-31), detectable HIV RNA (19; 9-31), and low CD4 cell count (13%; 4-21).
Interpretation: The substantial proportion of non-AIDS-defining cancers, myocardial infarction, end-stage liver disease, and end-stage renal disease outcomes that could be prevented with interventions on traditional risk factors elevates the importance of screening for these risk factors, improving the effectiveness of prevention (or modification) of these risk factors, and creating sustainable care models to implement such interventions during the decades of life of adults living with HIV who are receiving care.
Funding: National Institutes of Health, US Centers for Disease Control and Prevention, the US Agency for Healthcare Research and Quality, the US Health Resources and Services Administration, the Canadian Institutes of Health Research, the Ontario Ministry of Health and Long Term Care, and the Government of Alberta.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
How do we preserve health among adults living with HIV?Lancet HIV. 2019 Feb;6(2):e69-e70. doi: 10.1016/S2352-3018(18)30336-9. Epub 2019 Jan 22. Lancet HIV. 2019. PMID: 30683626 No abstract available.
References
-
- Friis-Møller N, Weber R, Reiss P, et al. Cardiovascular disease risk factors in HIV patients – association with antiretroviral therapy. Results from the DAD study. AIDS. 2003. May 23;17(8):1179–1193. - PubMed
-
- Sulkowski MS, Moore RD, Mehta SH, Chaisson RE, Thomas DL. Hepatitis C and progression of HIV disease. JAMA. 2002. July 10;288(2): 199–206. - PubMed
Publication types
MeSH terms
Grants and funding
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- U54 MD007587/MD/NIMHD NIH HHS/United States
- U01 AI037613/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- K24 DA035684/DA/NIDA NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- N01 CP001004/CP/NCI NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- F31 AI124794/AI/NIAID NIH HHS/United States
- P30 MH062246/MH/NIMH NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- U01 AI037984/AI/NIAID NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- K23 EY013707/EY/NEI NIH HHS/United States
- R01 CA165937/CA/NCI NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- P30 CA006973/CA/NCI NIH HHS/United States
- R01 DA026770/DA/NIDA NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- K24 DA000432/DA/NIDA NIH HHS/United States
- CBR-94036/CIHR/Canada
- R24 AG044325/AG/NIA NIH HHS/United States
- U01 DA036935/DA/NIDA NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- U01 HL146201/HL/NHLBI NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- CBR-86906/CIHR/Canada
- P30 AI110527/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- K24 AI118591/AI/NIAID NIH HHS/United States
- K24 AI065298/AI/NIAID NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- U01 AA013566/AA/NIAAA NIH HHS/United States
- N02 CP055504/CP/NCI NIH HHS/United States
- KL2 TR002317/TR/NCATS NIH HHS/United States
- UL1 TR000083/TR/NCATS NIH HHS/United States
- R01 HL126538/HL/NHLBI NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- TGF-96118 /CIHR/Canada
- KL2 TR000421/TR/NCATS NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- U01 AI103390/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- HCP-97105 /CIHR/Canada
- UL1 TR000004/TR/NCATS NIH HHS/United States
- P30 AI117943/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- F31 DA037788/DA/NIDA NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- R01 AG053100/AG/NIA NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
