

Imaging features of adrenal masses
- PMID: 30684056
- PMCID: PMC6349247
- DOI: 10.1186/s13244-019-0688-8
Imaging features of adrenal masses
Abstract
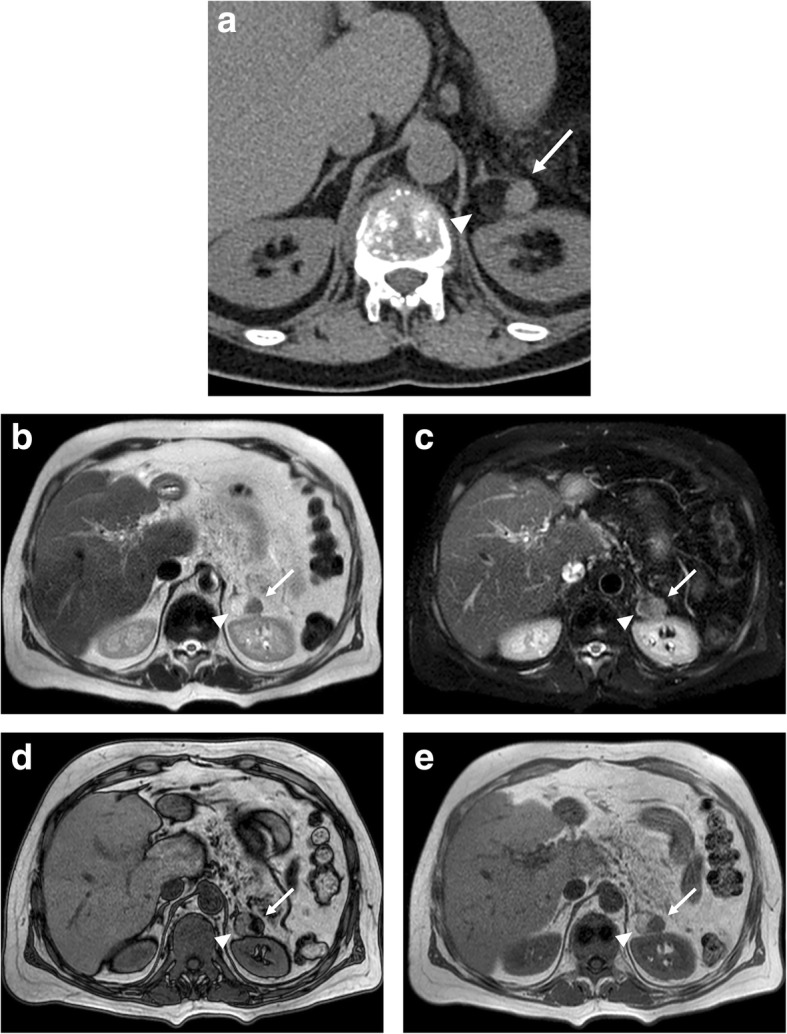
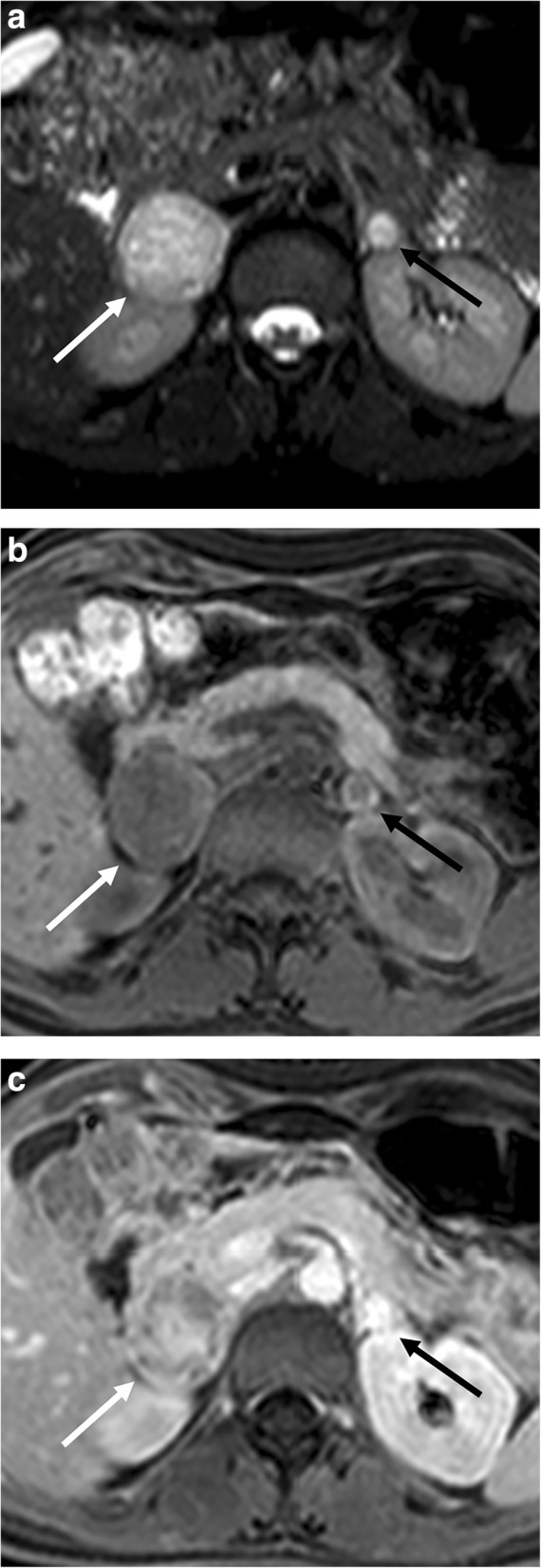
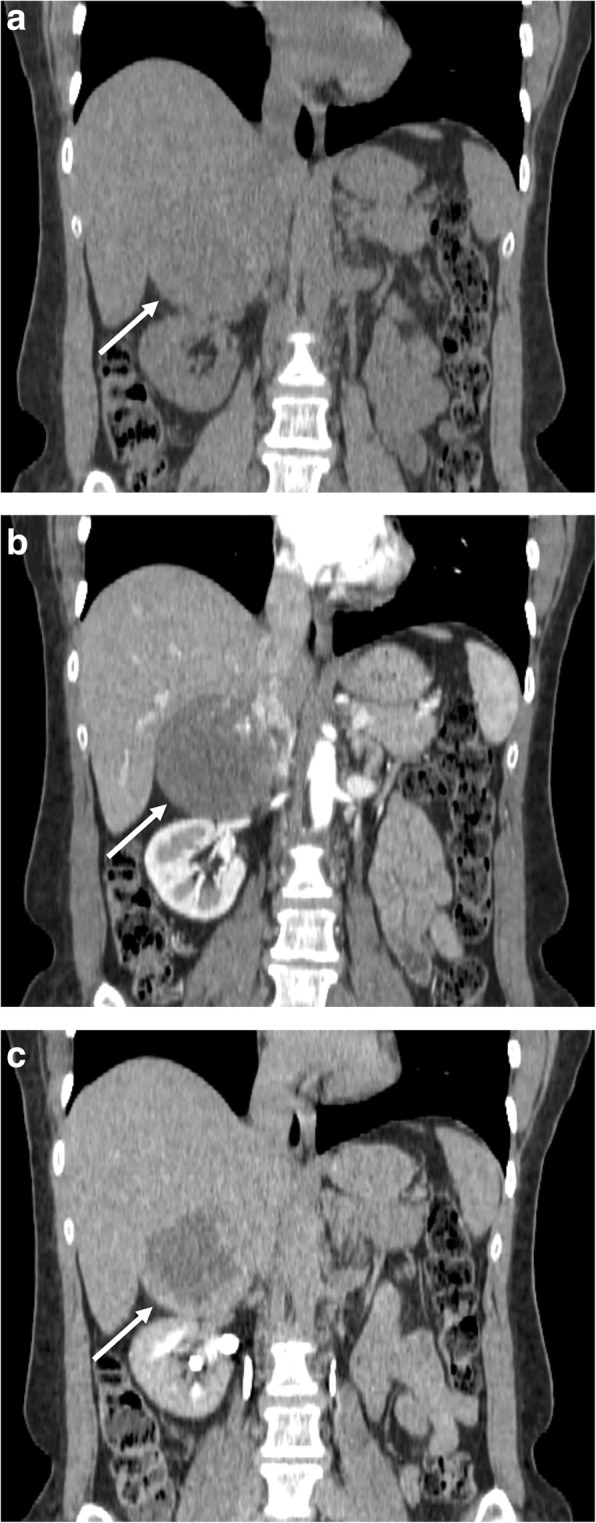
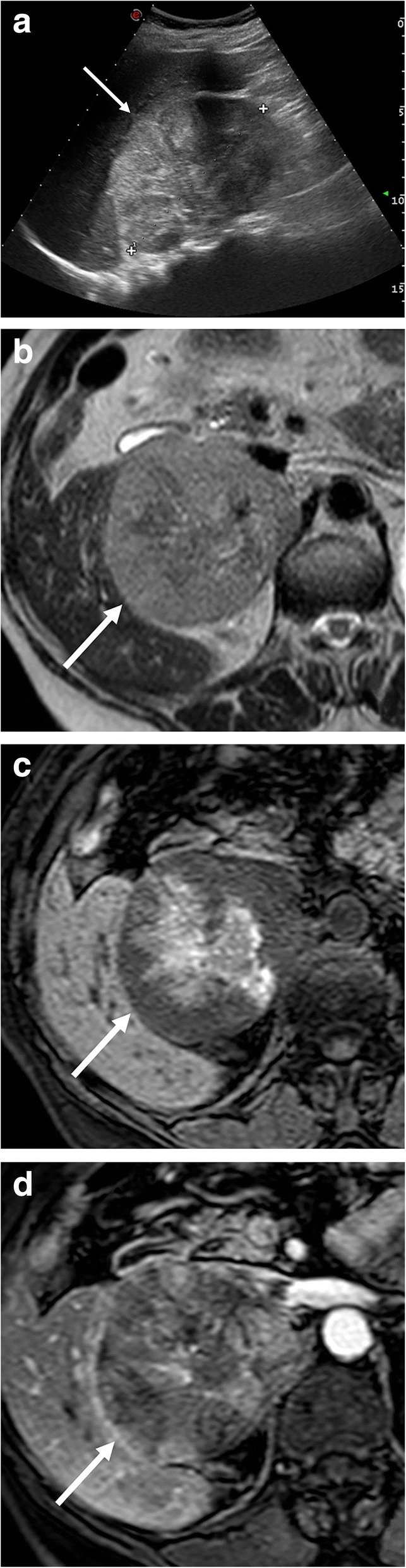
The widespread use of imaging examinations has increased the detection of incidental adrenal lesions, which are mostly benign and non-functioning adenomas. The differentiation of a benign from a malignant adrenal mass can be crucial especially in oncology patients since it would greatly affect treatment and prognosis. In this setting, imaging plays a key role in the detection and characterization of adrenal lesions, with several imaging tools which can be employed by radiologists. A thorough knowledge of the imaging features of adrenal masses is essential to better characterize these lesions, avoiding a misinterpretation of imaging findings, which frequently overlap between benign and malignant conditions, thus helping clinicians and surgeons in the management of patients. The purpose of this paper is to provide an overview of the main imaging features of adrenal masses and tumor-like conditions recalling the strengths and weaknesses of imaging modalities commonly used in adrenal imaging.
Keywords: Adenoma; Adrenal; Chemical shift imaging; Computed tomography; Magnetic resonance imaging.
Conflict of interest statement
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Galia M, Albano D, Narese D et al (2016) Whole body MRI in patients with lymphoma: collateral findings. Radiol Med. 10.1007/s11547-016-0658-x - PubMed
-
- Mayo-Smith WW, Song JH, Boland GL, et al (2017) Management of incidental adrenal masses: a White Paper of the ACR Incidental Findings Committee. J Am Coll Radiol. 10.1016/j.jacr.2017.05.001 - PubMed
-
- Kebebew E (2017) Management of adrenal masses in children and adults. Springer. 10.1007/978-3-319-44136-8
-
- Johnson PT, Horton KM, Fishman EK (2009) Adrenal mass imaging with multidetector CT: pathologic conditions, pearls, and pitfalls. Radiographics. 10.1148/rg.295095027 - PubMed
