

A Unique Collateral Artery Development Program Promotes Neonatal Heart Regeneration
- PMID: 30686582
- PMCID: PMC6435282
- DOI: 10.1016/j.cell.2018.12.023
A Unique Collateral Artery Development Program Promotes Neonatal Heart Regeneration
Abstract
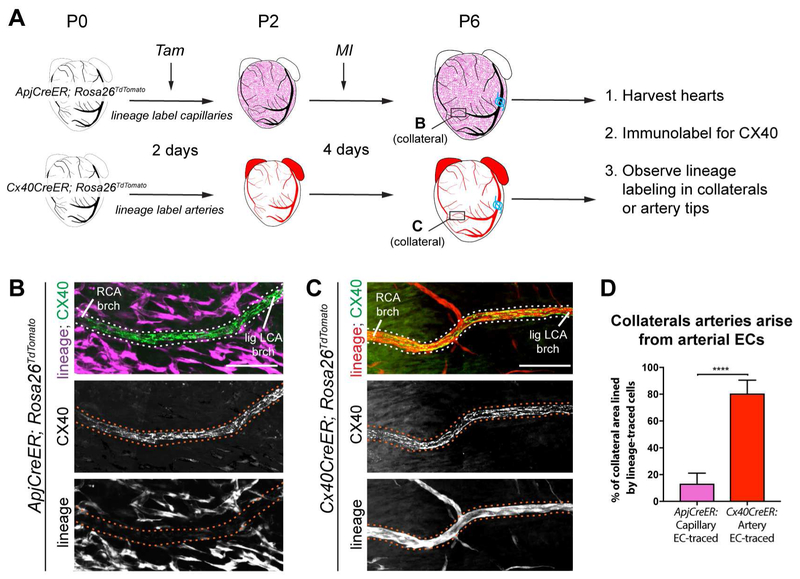
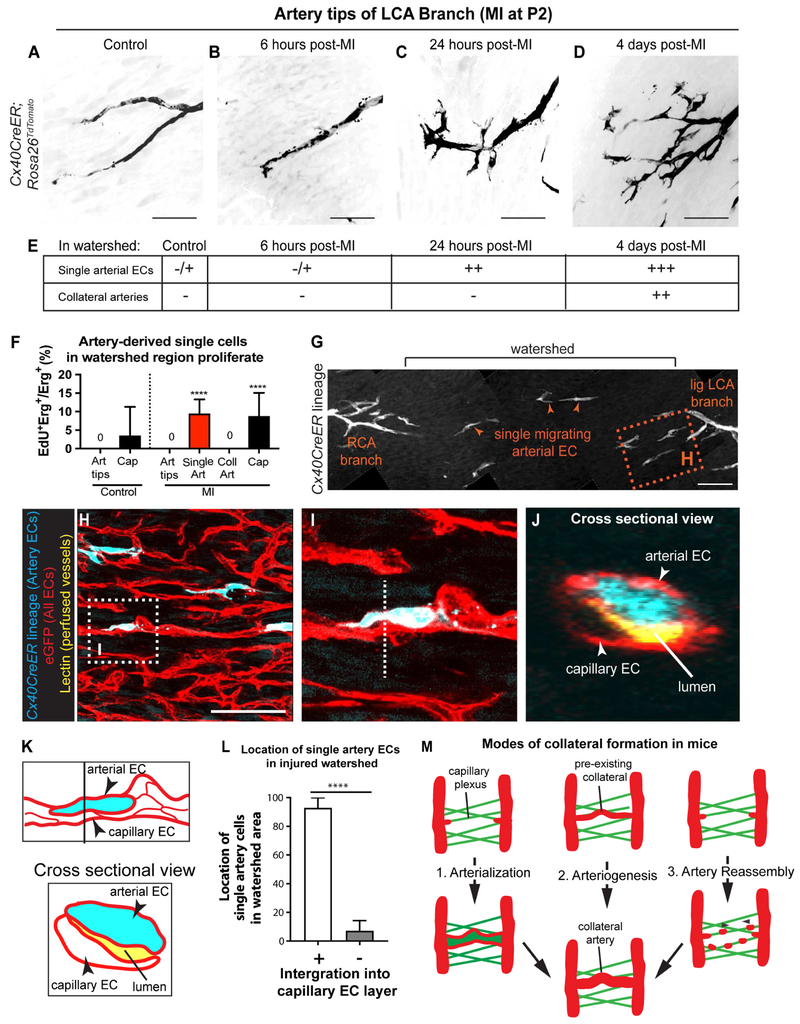
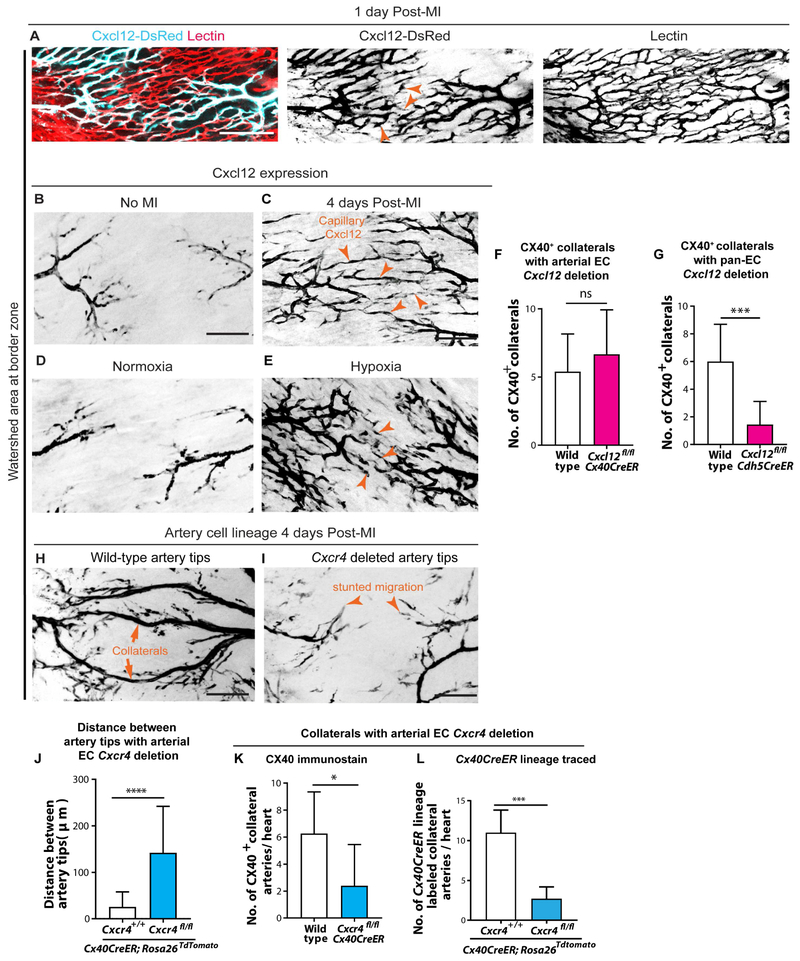
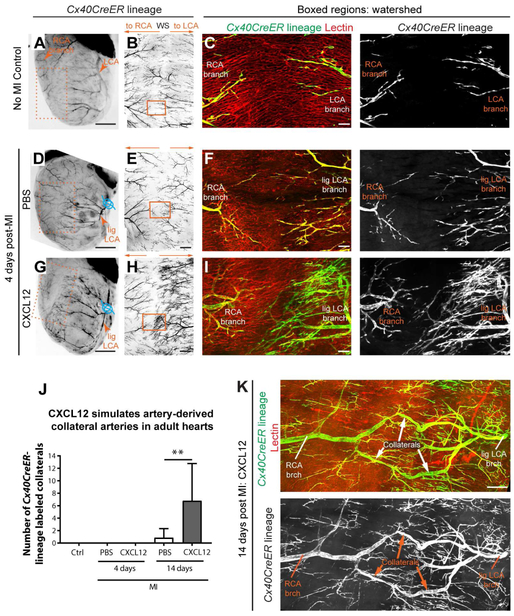
Collateral arteries are an uncommon vessel subtype that can provide alternate blood flow to preserve tissue following vascular occlusion. Some patients with heart disease develop collateral coronary arteries, and this correlates with increased survival. However, it is not known how these collaterals develop or how to stimulate them. We demonstrate that neonatal mouse hearts use a novel mechanism to build collateral arteries in response to injury. Arterial endothelial cells (ECs) migrated away from arteries along existing capillaries and reassembled into collateral arteries, which we termed "artery reassembly". Artery ECs expressed CXCR4, and following injury, capillary ECs induced its ligand, CXCL12. CXCL12 or CXCR4 deletion impaired collateral artery formation and neonatal heart regeneration. Artery reassembly was nearly absent in adults but was induced by exogenous CXCL12. Thus, understanding neonatal regenerative mechanisms can identify pathways that restore these processes in adults and identify potentially translatable therapeutic strategies for ischemic heart disease.
Keywords: CXCL12; arterialization; arteriogenesis; collateral arteries; endothelial cells; heart regeneration; myocardial infarction.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures



Comment in
-
A Watershed Finding for Heart Regeneration.Cell. 2019 Feb 21;176(5):947-949. doi: 10.1016/j.cell.2019.01.053. Cell. 2019. PMID: 30794778 Free PMC article.
References
-
- Abbott JD, Huang Y, Liu D, Hickey R, Krause DS, and Giordano FJ (2004). Stromal cell-derived factor-1alpha plays a critical role in stem cell recruitment to the heart after myocardial infarction but is not sufficient to induce homing in the absence of injury. Circulation 110, 3300–3305. - PubMed
-
- Askari AT, Unzek S, Popovic ZB, Goldman CK, Forudi F, Kiedrowski M, Rovner A, Ellis SG, Thomas JD, DiCorleto PE, et al. (2003). Effect of stromal-cell-derived factor 1 on stem-cell homing and tissue regeneration in ischaemic cardiomyopathy. Lancet 362, 697–703. - PubMed
-
- Baxter R, Hastings N, Law A, and Glass EJ. (2008). CXCL12 gene expression is upregulated by hypoxia and growth arrest but not by inflammatory cytokines in rheumatoid synovial fibroblasts. Anim. Genet 39, 561–563.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
