

Glioblastoma Treatment with Temozolomide and Bevacizumab and Overall Survival in a Rural Tertiary Healthcare Practice
- PMID: 30687753
- PMCID: PMC6330814
- DOI: 10.1155/2018/6204676
Glioblastoma Treatment with Temozolomide and Bevacizumab and Overall Survival in a Rural Tertiary Healthcare Practice
Abstract
Background: The efficacy of temozolomide (TMZ) chemotherapy for treating newly diagnosed glioblastoma (GBM), a primary brain tumor with short survival, was demonstrated in a clinical trial in 2005, and since then, the standard-of-care for newly diagnosed GBM has been maximal safe surgery followed by 60 Gray of radiation with concomitant and adjuvant TMZ (standard radiotherapy and TMZ). In 2009, clinical trials also reported on the efficacy of bevacizumab for treating recurrent GBM. We performed a retrospective cohort study to evaluate the impact of treatment regimens on overall survival for patients with GBM at a rural tertiary healthcare practice.
Methods: We retrospectively reviewed the medical records of 307 consecutive, newly diagnosed GBM patients at one institution between 1995 and 2012 and assessed treatment patterns. We also compared overall survival according to the treatment received.
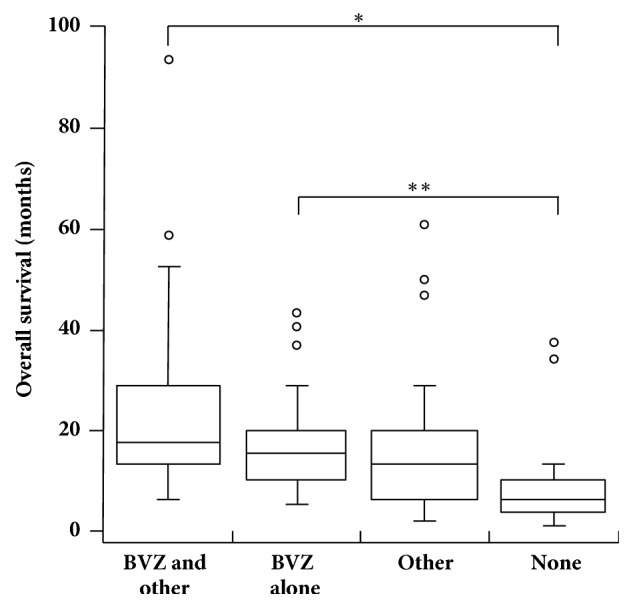
Results: Only 0.6% (1/163) of patients diagnosed before 2005 received standard radiotherapy and TMZ versus 36.1% (52/144) of patients diagnosed since 2005 (P < 0.0001). For patients who received standard radiotherapy and TMZ, the median overall survival was 17.0 months versus 7.0 months for patients who received 60 Gray of radiation but no chemotherapy (P = 0.0000078). The median overall survival was 15.4 months in the 19 patients treated with bevacizumab monotherapy at first GBM recurrence versus 6.8 months in the 32 patients with no treatment at first GBM recurrence (P = 0.00015), but patients who received bevacizumab were younger and more likely to have had a surgical resection and 60 Gray of radiation at diagnosis.
Conclusions: TMZ and bevacizumab therapies were rapidly adopted in a rural tertiary healthcare setting, and patients who received these treatments had increased overall survival. However, advantageous prognostic factors in patients who received bevacizumab at recurrence may have influenced the extent of the increase in overall survival attributed to this treatment.
Figures
Similar articles
-
Survival benefits of hypofractionated radiotherapy combined with temozolomide or temozolomide plus bevacizumab in elderly patients with glioblastoma aged ≥ 75 years.Radiat Oncol. 2019 Nov 12;14(1):200. doi: 10.1186/s13014-019-1389-7. Radiat Oncol. 2019. PMID: 31718669 Free PMC article.
-
Dexamethasone administration during definitive radiation and temozolomide renders a poor prognosis in a retrospective analysis of newly diagnosed glioblastoma patients.Radiat Oncol. 2015 Oct 31;10:222. doi: 10.1186/s13014-015-0527-0. Radiat Oncol. 2015. PMID: 26520780 Free PMC article.
-
Effectiveness of temozolomide treatment used at the same time with radiotherapy and adjuvant temozolomide; concomitant therapy of glioblastoma multiforme: multivariate analysis and other prognostic factors.J Neurosurg Sci. 2010 Mar;54(1):7-19. J Neurosurg Sci. 2010. PMID: 20436394
-
A Systematic Review and Meta-Analysis on the Effectiveness of Radiotherapy and Temozolomide Treatment With or Without Bevacizumab in Patients With Glioblastoma Multiforme.Neurol India. 2024 Jul 1;72(4):700-707. doi: 10.4103/neurol-india.Neurol-India-D-23-00346. Epub 2024 Aug 31. Neurol India. 2024. PMID: 39216020
-
The Evolving Role of Tumor Treating Fields in Managing Glioblastoma: Guide for Oncologists.Am J Clin Oncol. 2018 Feb;41(2):191-196. doi: 10.1097/COC.0000000000000395. Am J Clin Oncol. 2018. PMID: 28832384 Free PMC article. Review.
Cited by
-
AHR, a novel inhibitory immune checkpoint receptor, is a potential therapeutic target for chemoresistant glioblastoma.J Cancer Res Clin Oncol. 2023 Sep;149(12):9705-9720. doi: 10.1007/s00432-023-04894-w. Epub 2023 May 26. J Cancer Res Clin Oncol. 2023. PMID: 37233762 Free PMC article.
-
Involvement of cell shape and lipid metabolism in glioblastoma resistance to temozolomide.Acta Pharmacol Sin. 2023 Mar;44(3):670-679. doi: 10.1038/s41401-022-00984-6. Epub 2022 Sep 13. Acta Pharmacol Sin. 2023. PMID: 36100765 Free PMC article.
-
Transferrin Modified GSH Sensitive Hyaluronic Acid Derivative Micelle to Deliver HSP90 Inhibitors to Enhance the Therapeutic Efficacy of Brain Cancers.Cancers (Basel). 2021 May 14;13(10):2375. doi: 10.3390/cancers13102375. Cancers (Basel). 2021. PMID: 34069106 Free PMC article.
-
Surgery, Octreotide, Temozolomide, Bevacizumab, Radiotherapy, and Pegvisomant Treatment of an AIP Mutation‒Positive Child.J Clin Endocrinol Metab. 2019 Aug 1;104(8):3539-3544. doi: 10.1210/jc.2019-00432. J Clin Endocrinol Metab. 2019. PMID: 31125088 Free PMC article.
-
Mechanisms of temozolomide resistance in glioblastoma - a comprehensive review.Cancer Drug Resist. 2021;4(1):17-43. doi: 10.20517/cdr.2020.79. Epub 2021 Mar 19. Cancer Drug Resist. 2021. PMID: 34337348 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
