

A current understanding of drug-induced QT prolongation and its implications for anticancer therapy
- PMID: 30689740
- PMCID: PMC7967705
- DOI: 10.1093/cvr/cvz013
A current understanding of drug-induced QT prolongation and its implications for anticancer therapy
Abstract
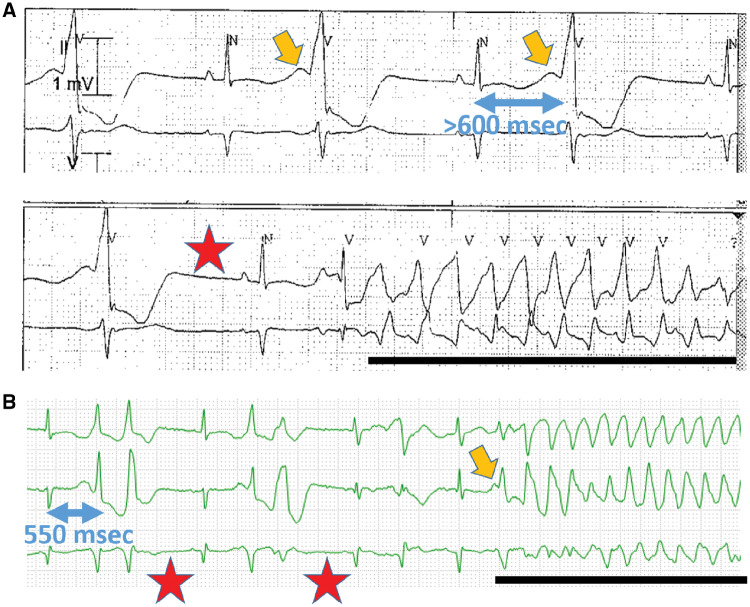
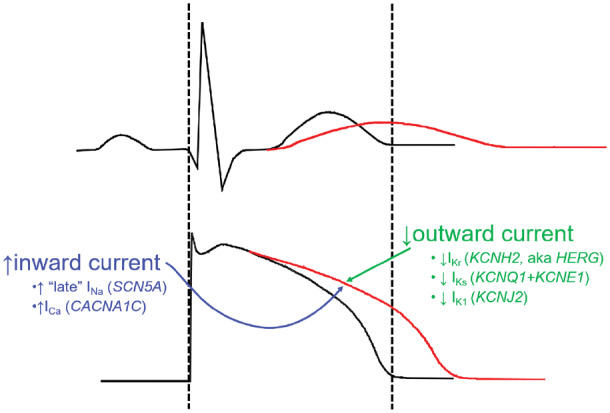
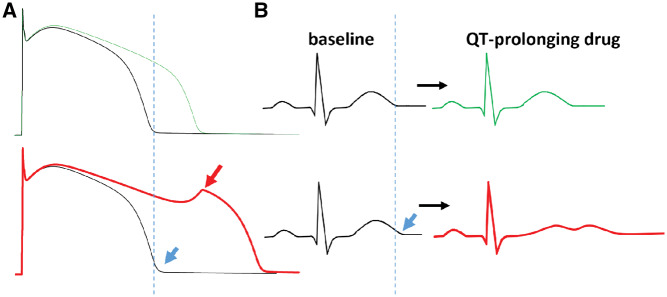
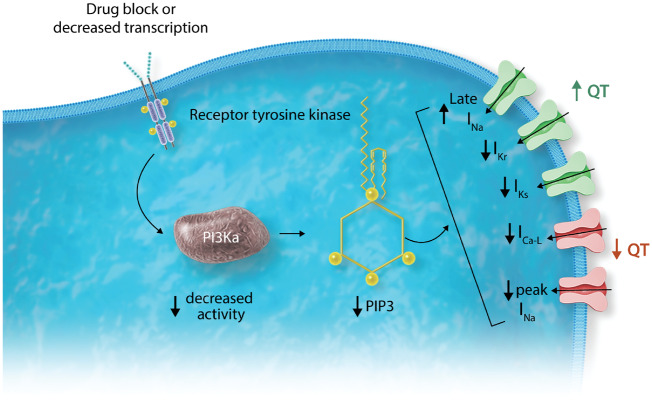
The QT interval, a global index of ventricular repolarization, varies among individuals and is influenced by diverse physiologic and pathophysiologic stimuli such as gender, age, heart rate, electrolyte concentrations, concomitant cardiac disease, and other diseases such as diabetes. Many drugs produce a small but reproducible effect on QT interval but in rare instances this is exaggerated and marked QT prolongation can provoke the polymorphic ventricular tachycardia 'torsades de pointes', which can cause syncope or sudden cardiac death. The generally accepted common mechanism whereby drugs prolong QT is block of a key repolarizing potassium current in heart, IKr, generated by expression of KCNH2, also known as HERG. Thus, evaluation of the potential that a new drug entity may cause torsades de pointes has relied on exposure of normal volunteers or patients to drug at usual and high concentrations, and on assessment of IKr block in vitro. More recent work, focusing on anticancer drugs with QT prolonging liability, is defining new pathways whereby drugs can prolong QT. Notably, the in vitro effects of some tyrosine kinase inhibitors to prolong cardiac action potentials (the cellular correlate of QT) can be rescued by intracellular phosphatidylinositol 3,4,5-trisphosphate, the downstream effector of phosphoinositide 3-kinase. This finding supports a role for inhibition of this enzyme, either directly or by inhibition of upstream kinases, to prolong QT through mechanisms that are being worked out, but include enhanced inward 'late' sodium current during the plateau of the action potential. The definition of non-IKr-dependent pathways to QT prolongation will be important for assessing risk, not only with anticancer therapies but also with other QT prolonging drugs and for generating a refined understanding how variable activity of intracellular signalling systems can modulate QT and associated arrhythmia risk.
Keywords: Arrhythmia; Cardio-oncology; PI3 Kinase; QT Prolongation; Torsades de pointes.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2019. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Roden DM. Drug-induced prolongation of the QT Interval. N Engl J Med 2004;350:1013–1022. - PubMed
-
- Choy AM, Darbar D, Dell'Orto S, Roden DM. Exaggerated QT prolongation after cardioversion of atrial fibrillation. J Am Coll Cardiol 1999;34:396–401. - PubMed
-
- Astrom-Lilja C, Odeberg JM, Ekman E, Hagg S. Drug-induced torsades de pointes: a review of the Swedish pharmacovigilance database. Pharmacoepidemiol drug safety 2008;17:587–592. - PubMed
-
- Lazzerini PE, Laghi-Pasini F, Bertolozzi I, Morozzi G, Lorenzini S, Simpatico A, Selvi E, Bacarelli MR, Finizola F, Vanni F, Lazaro D, Aromolaran A, El Sherif N, Boutjdir M, Capecchi PL. Systemic inflammation as a novel QT-prolonging risk factor in patients with torsades de pointes. Heart 2017;103:1821–1829. - PubMed
