

Planned delivery or expectant management for late preterm pre-eclampsia: study protocol for a randomised controlled trial (PHOENIX trial)
- PMID: 30691508
- PMCID: PMC6350286
- DOI: 10.1186/s13063-018-3150-1
Planned delivery or expectant management for late preterm pre-eclampsia: study protocol for a randomised controlled trial (PHOENIX trial)
Abstract
Background: Pre-eclampsia is a pregnancy disorder, characterised by hypertension and multisystem complications in the mother. The adverse outcomes of pre-eclampsia include severe hypertension, stroke, renal and hepatic injury, haemorrhage, fetal growth restriction and even death. The optimal time to instigate delivery to prevent morbidity when pre-eclampsia occurs between 34 and 37 weeks' gestation, without increasing problems related to infant immaturity or complications, remains unclear.
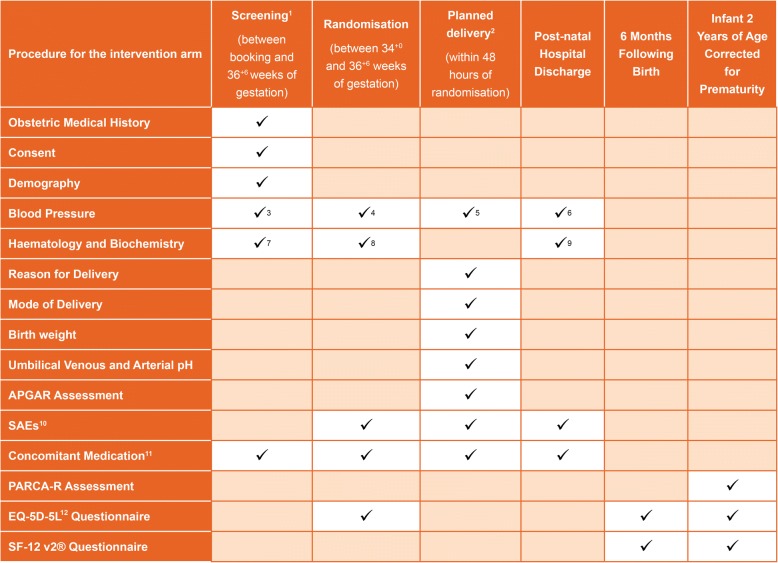
Methods/design: The PHOENIX trial is a non-masked, randomised controlled trial, comparing planned early delivery (with initiation of delivery within 48 h of randomisation) with usual care (expectant management) in women with pre-eclampsia between 34+ 0 and 36+ 6 weeks' gestation. The primary objectives of the trial are to determine if planned delivery reduces adverse maternal outcomes, without increasing the short-term harm to infants (composite of perinatal deaths or neonatal unit admissions up to infant hospital discharge) or impacting long-term infant neurodevelopmental status at 2 years corrected age (Parent Report of Cognitive Abilities-Revised).
Discussion: Current practice in the UK at the time of trial commencement for management of pre-eclampsia varies by gestation. Previous trials have shown that in women with pre-eclampsia after 37 weeks of gestion, delivery is initiated, as maternal complications are reduced without increasing fetal risks. Prior to 34 weeks of gestation, usual management aims to prolong pregnancy for fetal benefit, unless severe complications occur, necessitating preterm delivery. This trial aims to address the uncertainty for women where the balance of benefits and risks of delivery compared to expectant management are uncertain. Previous trials in this area have been undertaken, but have not provided a definitive answer, and the research question remains active. The results of this trial are expected to influence clinical practice internationally, through direct adoption and by incorporation into guidelines in countries with similar settings.
Trial registration: ISRCTN01879376 . Registered on 25 November 2013.
Keywords: Pre-eclampsia; hypertension; perinatal; pregnancy.
Conflict of interest statement
Ethics approval and consent to participate
The study will start only after gaining approval from an NHS-registered REC. Additionally, approval of the appropriate trust research and development office will be sought for individual trial sites. The chief investigator or their delegate will submit and, where necessary, obtain approval from the REC and the appropriate trust research and development offices for any substantial amendments. All protocol modifications will be communicated promptly to sites once approved by the sponsor and the REC. Written informed consent will be obtained by the principal investigator or another study doctor with delegated authority.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Comment in
-
Long-term cardiovascular health after stopping pre-eclampsia.Lancet. 2019 Sep 28;394(10204):1120-1121. doi: 10.1016/S0140-6736(19)31993-2. Epub 2019 Aug 28. Lancet. 2019. PMID: 31472929 No abstract available.
References
-
- Churchill D, et al. Interventionist versus expectant care for severe pre-eclampsia between 24 and 34 weeks' gestation. Cochrane Database Syst Rev. 2013;7:CD003106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
