Sternoclavicular Joint Graft in Temporomandibular Joint Reconstruction for Ankylosis
- PMID: 30693248
- PMCID: PMC6327794
- DOI: 10.4103/ams.ams_209_17
Sternoclavicular Joint Graft in Temporomandibular Joint Reconstruction for Ankylosis
Abstract
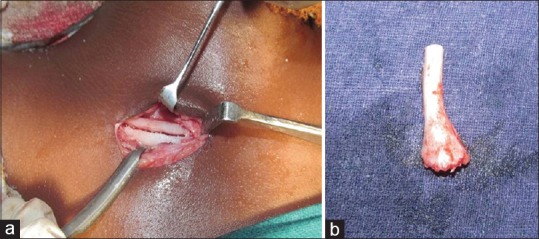
Background: Temporomandibular joint ankylosis is one of the most distressing clinical condition resulting in loss of jaw function and impairment of growth. Ankylosis is a greek word meaning "Stiff Joint". It is observed that in humans the Sternoclavicular joint and Temporomandibular joint are similar morphologically and histologically as they are the only two synovial joints covered with fibrocartilage. This similarity of the joints have encouraged the surgeons to use SCG as an alternative to costochondral grafts.
Aims: The purpose of this article was to evaluate the feasibility of using sternoclavicular graft for TMJ reconstruction in TMJ ankylosis patients and to also assess this technique in restoration of mandibular movement, function and growth of the mandible.
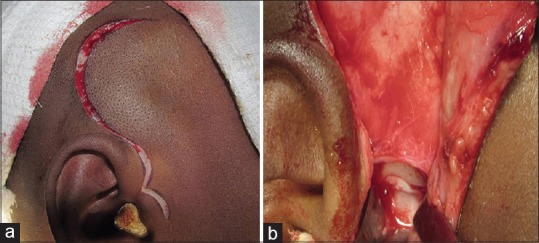
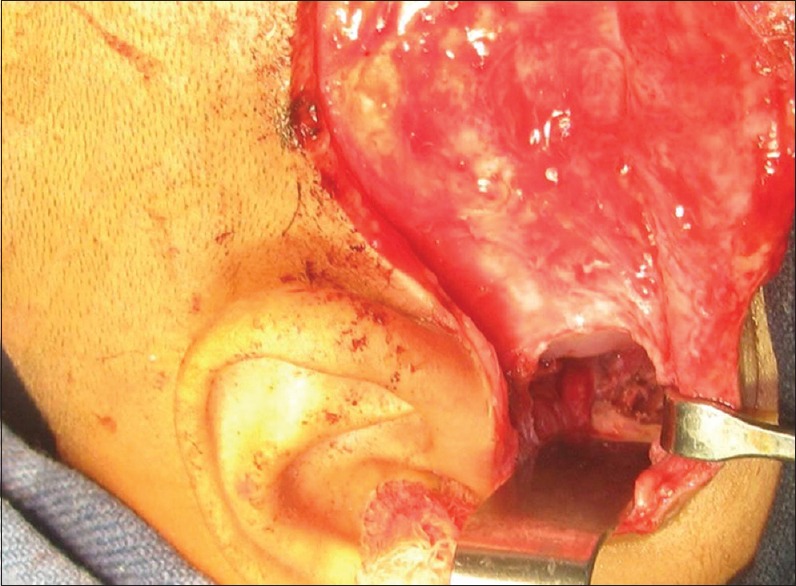
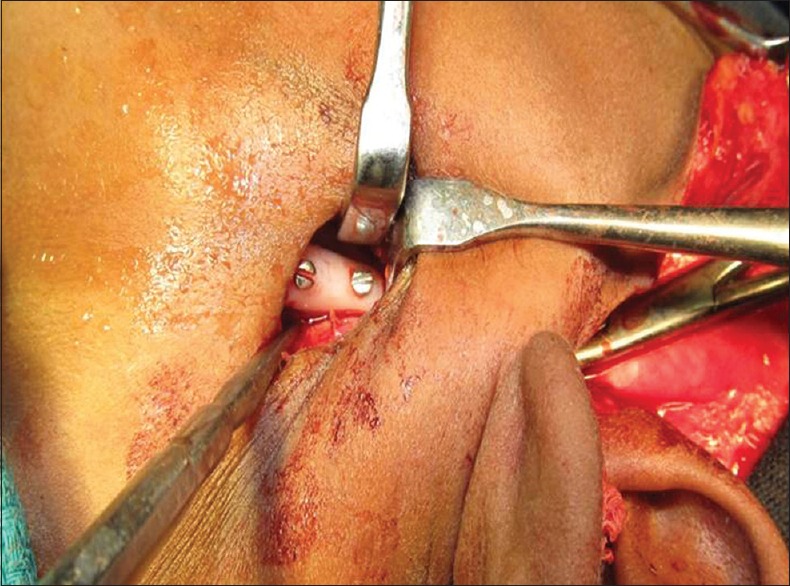
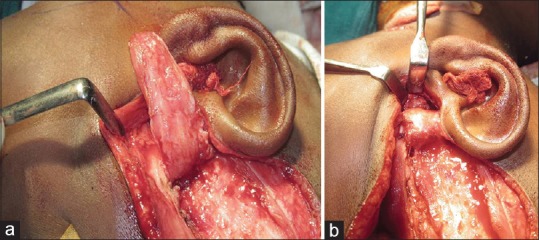
Settings and design: This retrospective study was conducted in 10 patients with unilateral TMJ ankylosiswho had undergone Interpositional arthroplasty with temporalis fascia and reconstruction of ramus condyle unit with sternoclavicular graft.
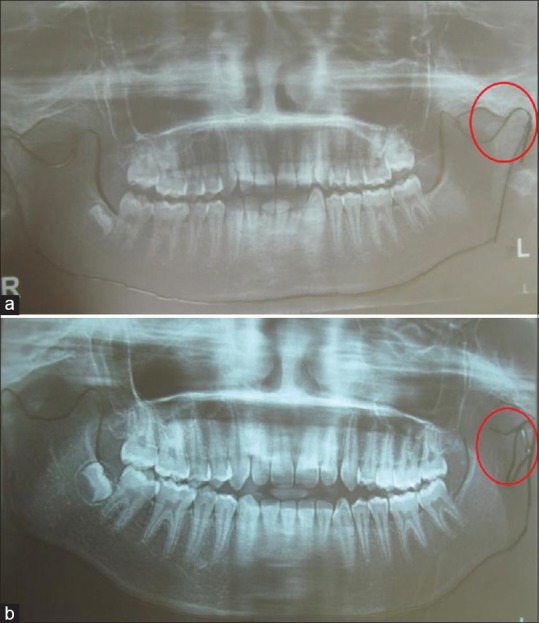
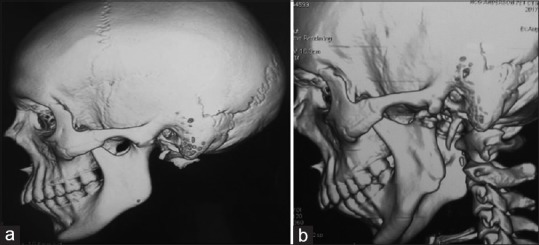
Methods and material: Ten patients(8 male and 2 female) with unilateral TMJ ankylosis within the growth period were included in the study. Clinical parameters assessed were maximal incisor opening, lateral excursion and protrusive movements.,ramus height,wound infection, donor sitemorbidity, evidence of neurological deficit in both donor and recipient site. Pre and post operative radiographic analysis of graft in relation to glenoid fossa and ramus of mandible was also done and donor site regeneration was also assessed.
Statistical analysis used: The data were analysed using SPSS version 20 (IBM Corporation, SPPSInc; Chicago, IL, USA). Paired T test was used to compare the pre operative and post operativelaterotrusive, protrusive movements and the height of the ramus of the mandible. Repeated measures ANOVA was used to analyse the mouth opening pre operatively ,immediate post operatively and a after 5- year follow up.
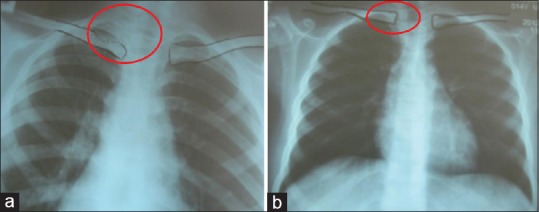
Results: The mean post operative mouth opening achieved was 28.9+_7.57mm with reankylosis in two patients. The mean laterotrusive and protrusive movements were 5.2 +_2.82mm and 2.2 +_.78 mm respectively postoperatively on a five year follow up. There was a 6.2 +_2.57mm increase in ramus height. The sternoclavicular graft had integrated and remodelled satisfactorily in eight patients. There was no change in the body length or midline deviation. Regarding the healing of the donor site there was a complete regeneration of clavicle within one year, however there was a incidence of clavicle fracture in one patient. The shoulder movements were normal in all patients.
Conclusions: The reconstruction of TMJ with SCG has proved to be successful in this study. With an impressive success rate, the sternoclavicular graft could become a versatile and viable alternative to the surgeons in reconstruction of TMJ as it is relatively simple to carry out with minimal complications and good results.
Keywords: Ankylosis; sternoclavicular graft; temporomandibular joint.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Valentini V, Vetrano S, Agrillo A, Torroni A, Fabiani F, Iannetti G, et al. Surgical treatment of TMJ ankylosis: Our experience (60 cases) J Craniofac Surg. 2002;13:59–67. - PubMed
-
- Katsnelson A, Markiewicz MR, Keith DA, Dodson TB. Operative management of temporomandibular joint ankylosis: A systematic review and meta-analysis. J Oral Maxillofac Surg. 2012;70:531–6. - PubMed
-
- Vasconcelos BC, Porto GG, Bessa-Nogueira RV, Nascimento MM. Surgical treatment of temporomandibular joint ankylosis: Follow-up of 15 cases and literature review. Med Oral Patol Oral Cir Bucal. 2009;14:E34–8. - PubMed
-
- Ellis E, 3rd, Carlson DS. Histologic comparison of the costochondral, sternoclavicular, and temporomandibular joints during growth in Macaca mulatta. J Oral Maxillofac Surg. 1986;44:312–21. - PubMed
-
- Daniels S, Ellis E, 3rd, Carlson DS. Histologic analysis of costochondral and sternoclavicular grafts in the TMJ of the juvenile monkey. J Oral Maxillofac Surg. 1987;45:675–83. - PubMed