

A Guide to Yellow Oral Mucosal Entities: Etiology and Pathology
- PMID: 30693453
- PMCID: PMC6405798
- DOI: 10.1007/s12105-018-0977-4
A Guide to Yellow Oral Mucosal Entities: Etiology and Pathology
Abstract
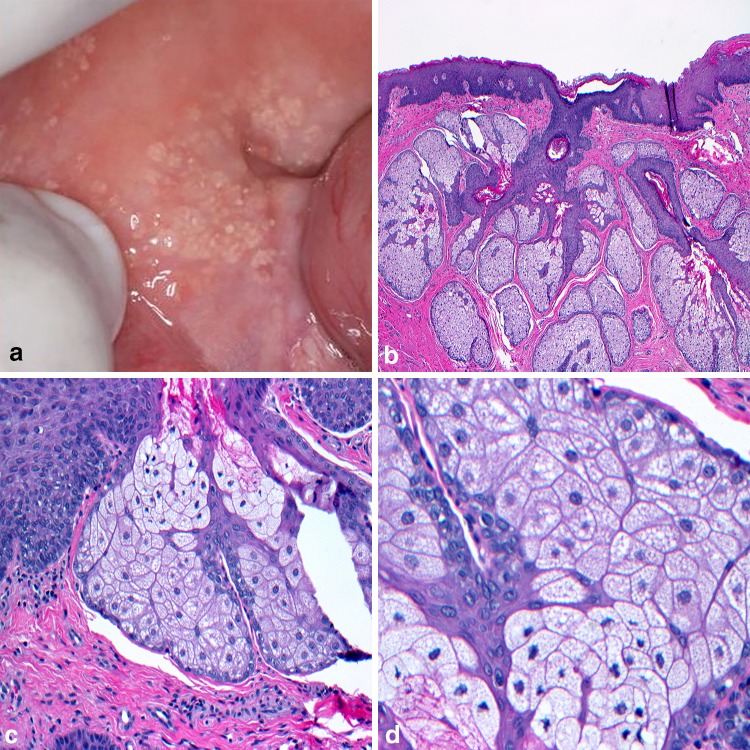
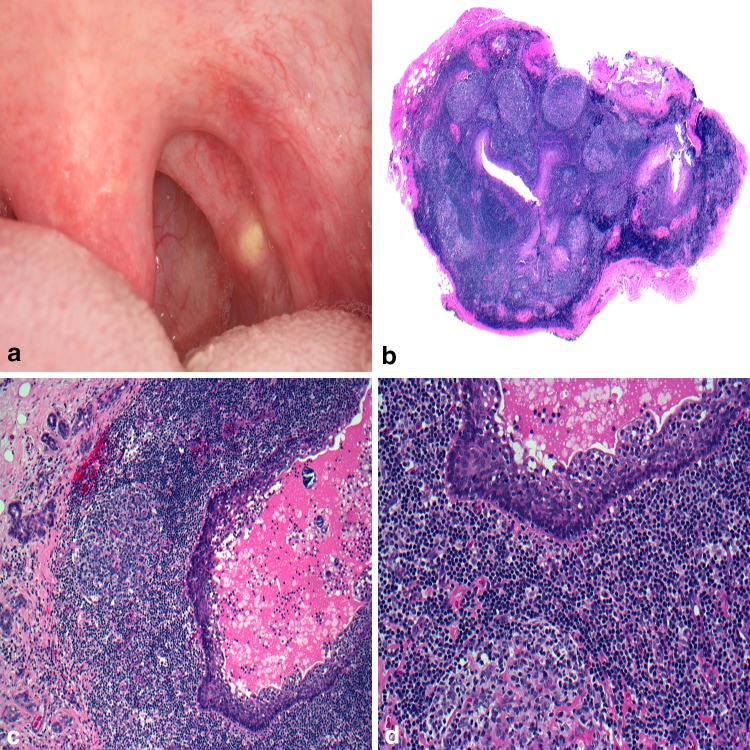
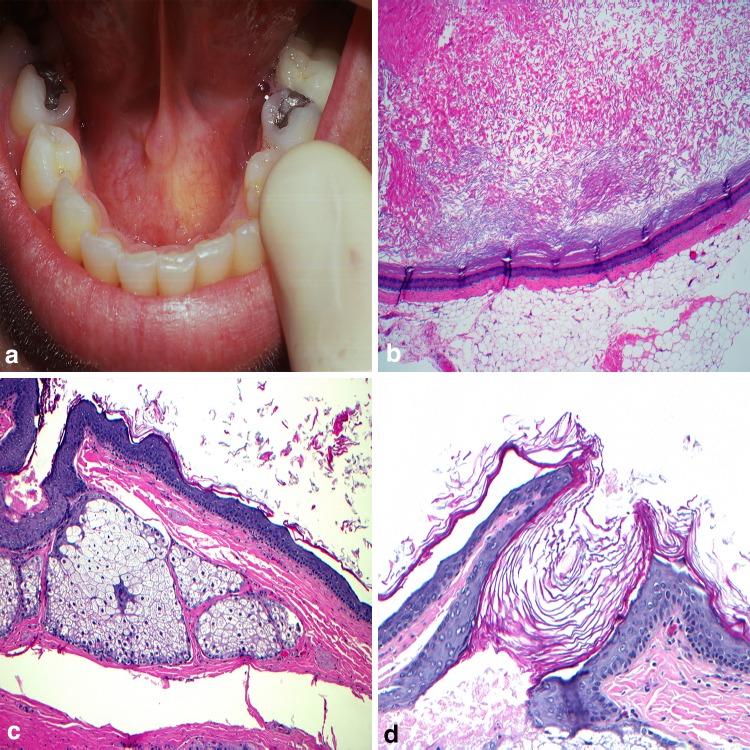
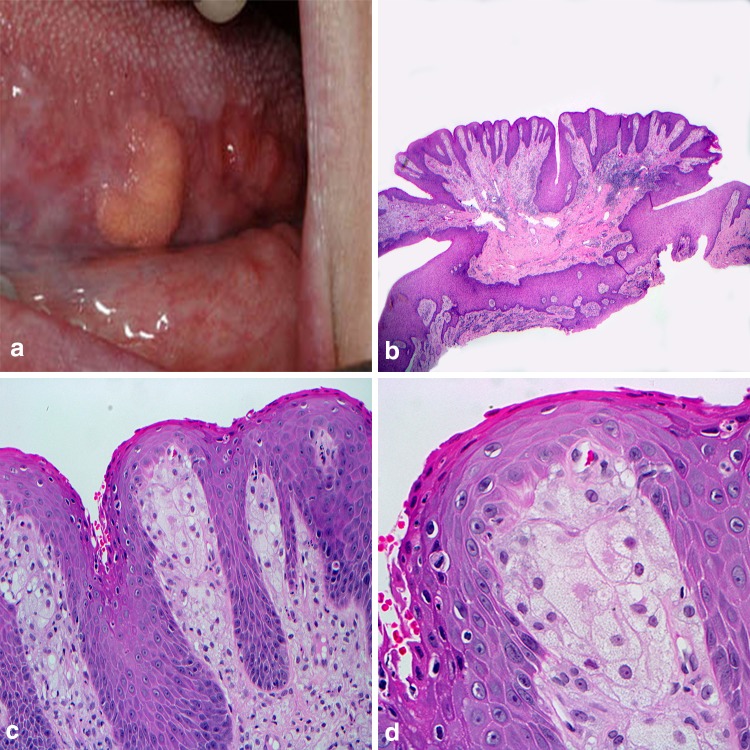
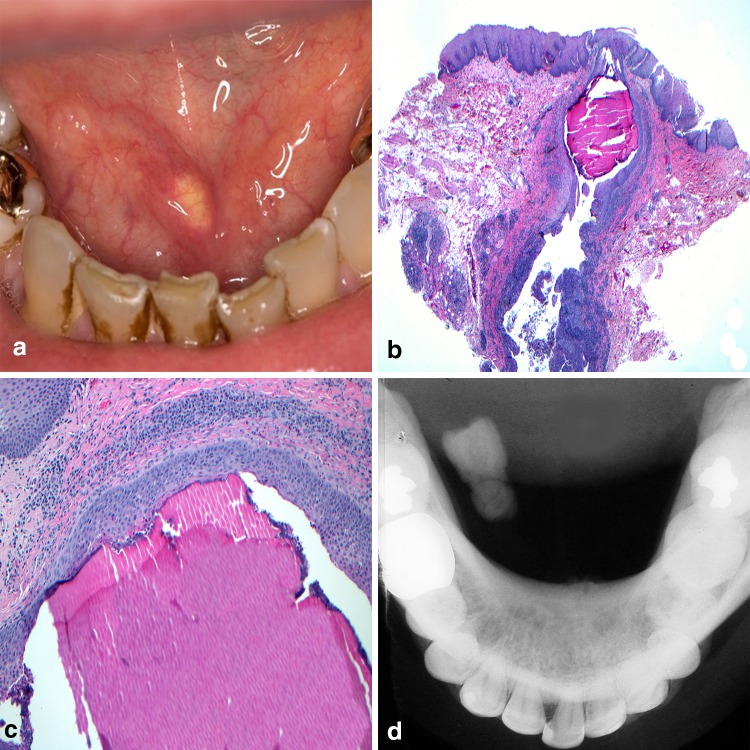
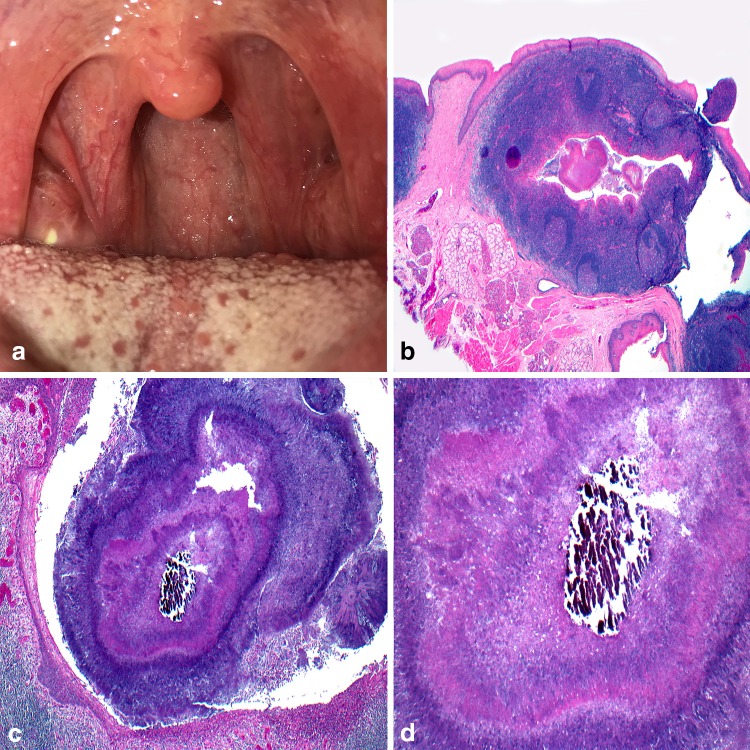
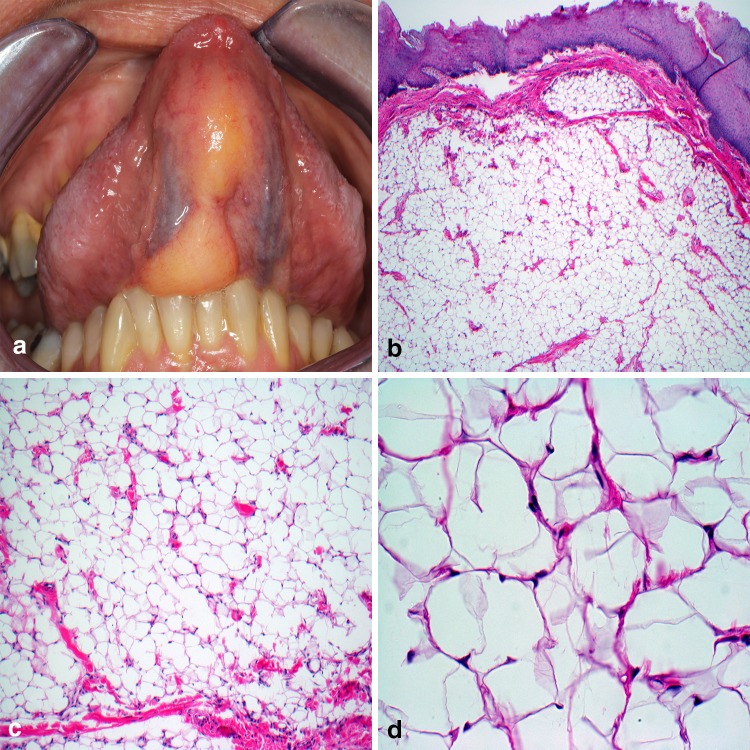
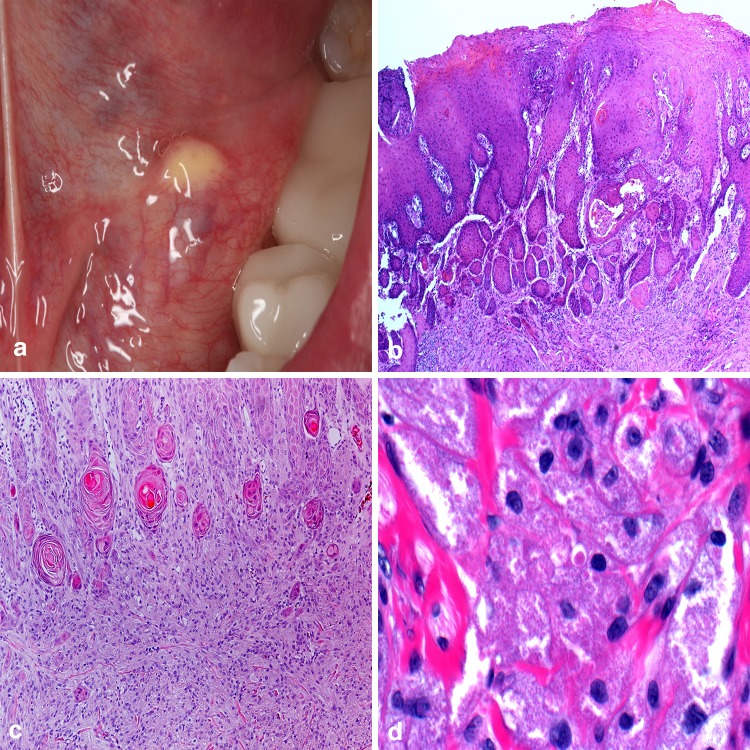
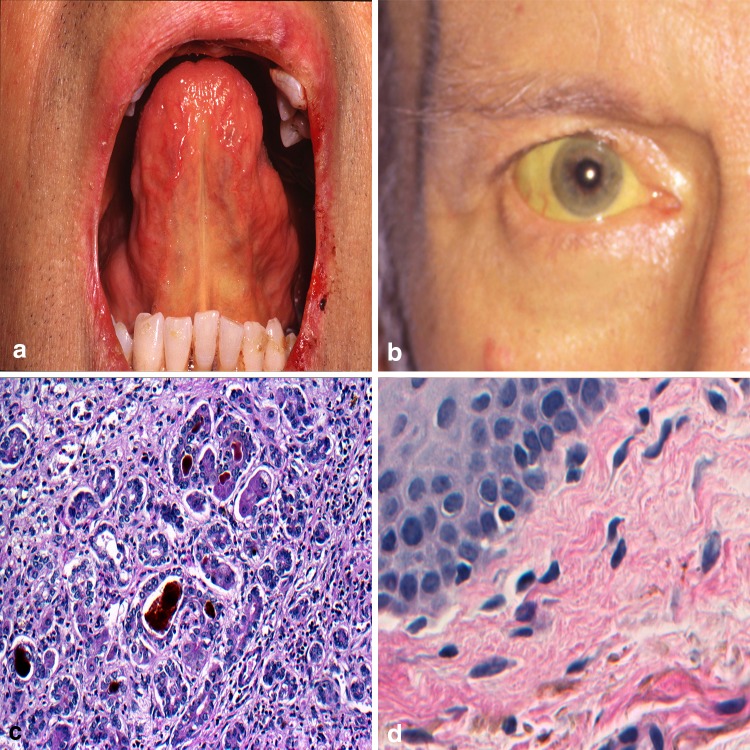
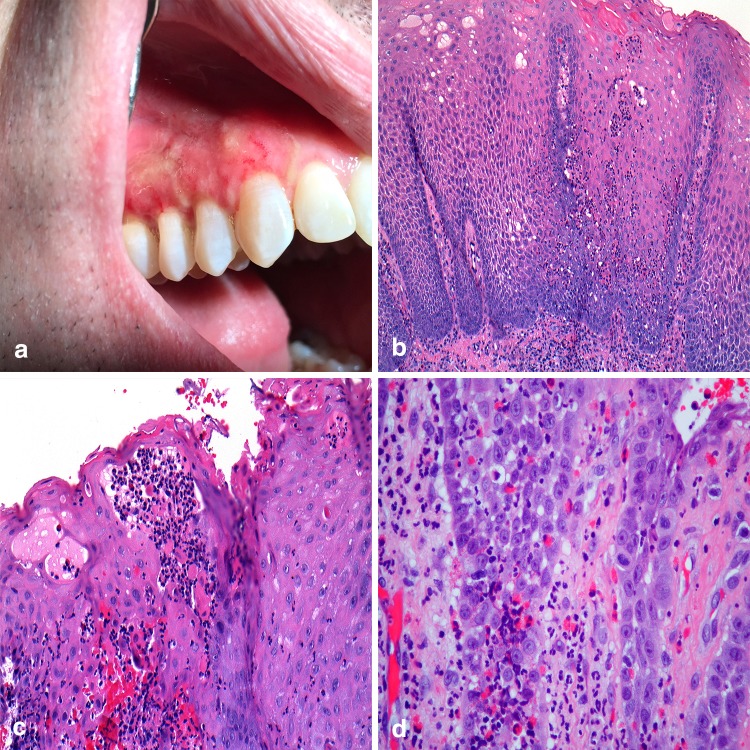
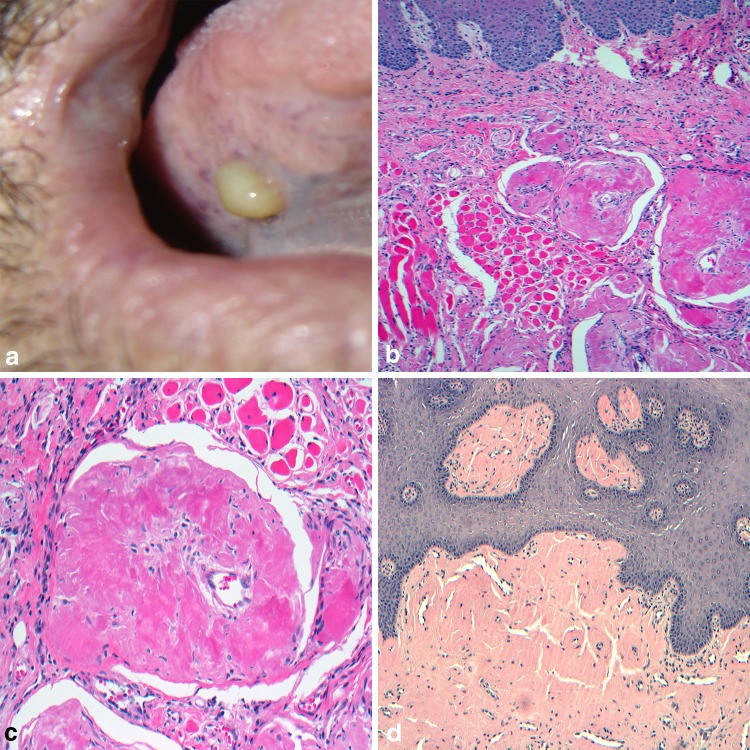
When faced with an uncertain clinical pathosis in the oral cavity, identifying the color of the mucosal lesion helps to narrow down a differential diagnosis. Although less common than red and white lesions, yellow lesions encompass a small group of distinct mucosal pathologic entities. Adipose tissue, lymphoid tissue, and sebaceous glands are naturally occurring yellow constituents of the oral cavity and become apparent with associated developmental or neoplastic lesions. Reactive and inflammatory lesions can create a yellow hue due to purulence, necrosis, and calcification. Some systemic diseases are known to deposit yellow bi-products such as amyloid or bilirubin into the oral mucosa of an affected person, and while not always yellow, unusual entities like verruciform xanthoma and granular cell tumor fall under the umbrella of yellow lesions given their occasional propensity to demonstration the color. This chapter aims to explore the unique group that is yellow lesions presenting in the oral mucosa.
Keywords: Mouth; Mucosal; Oral cavity; Oral manifestations; Systemic disease; Yellow.
Conflict of interest statement
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
As no human participants were involved in a study, informed consent was not required.
Figures
References
-
- Fordyce JA. A peculiar affection of the mucous membranes of the lips and the oral cavity. J Cutan Genito-Urin Dis. 1896;14:413–419.
-
- Neville BW, Damm DD, Allen CM, Chi AC. Developmental defects of the oral and maxillofacial region. Oral and maxillofacial pathology. 4. St. Louis: Elsevier; 2016. pp. 1–48.
-
- Batsakis JG, el-Naggar AK. Sebaceous lesion of salivary glands and oral cavity. Ann Otol Rhinol Laryngol. 1990;99:414–418. - PubMed
-
- Antonio N. Oral mucosa. Ten Cate’s oral histology. 9. St. Louis: Elsevier; 2017. pp. 260–288.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
