

Tongue Lumps and Bumps: Histopathological Dilemmas and Clues for Diagnosis
- PMID: 30693454
- PMCID: PMC6405789
- DOI: 10.1007/s12105-019-01005-5
Tongue Lumps and Bumps: Histopathological Dilemmas and Clues for Diagnosis
Abstract
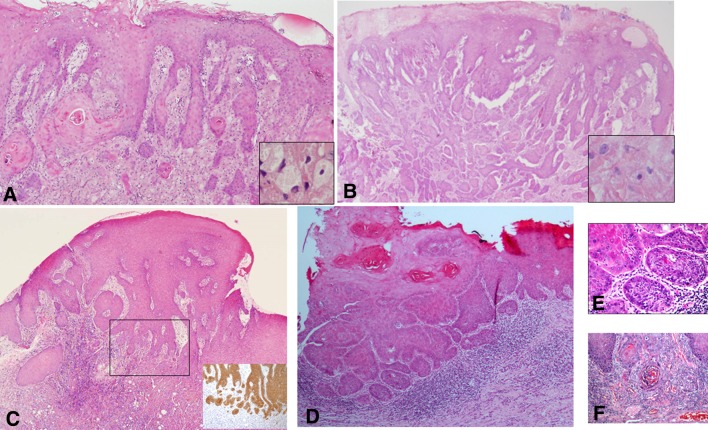
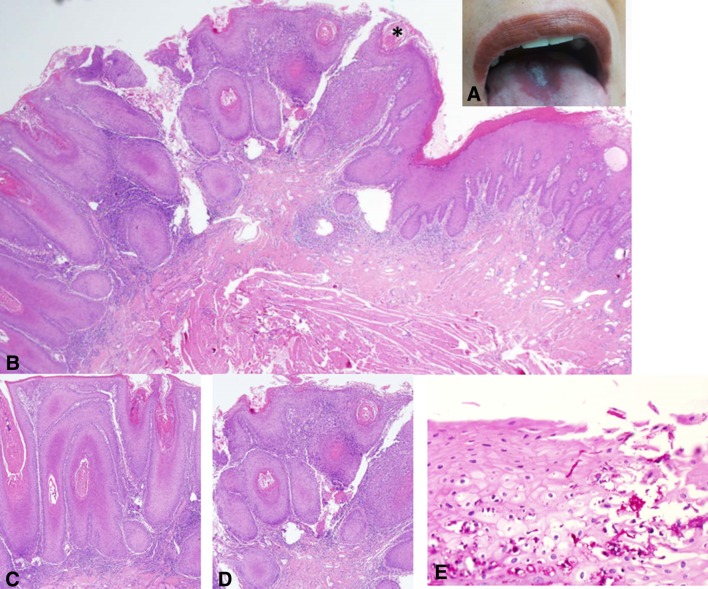
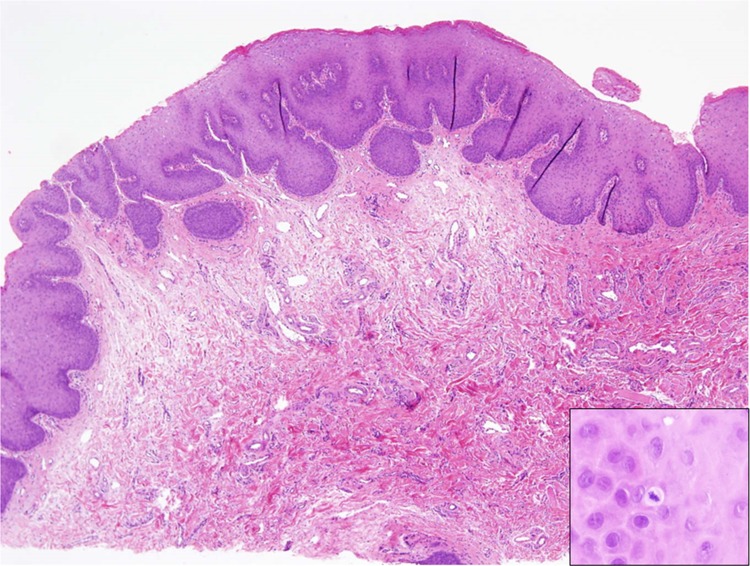
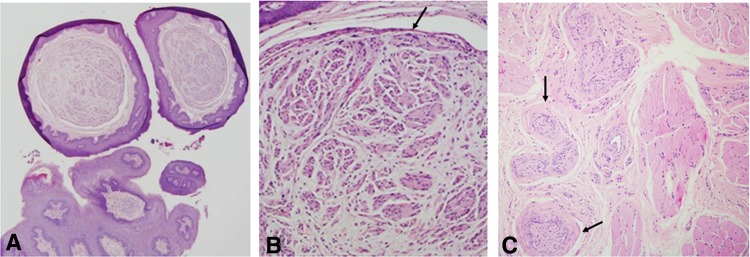
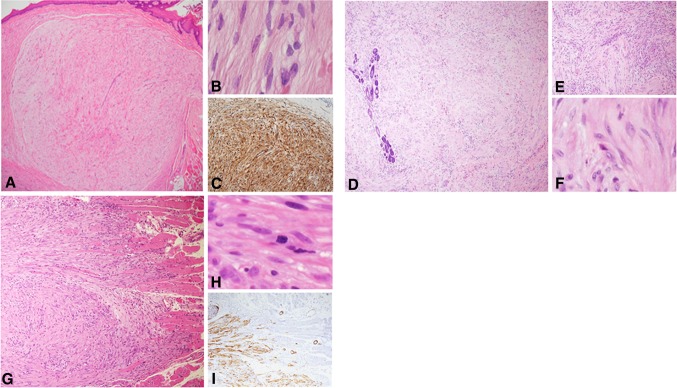
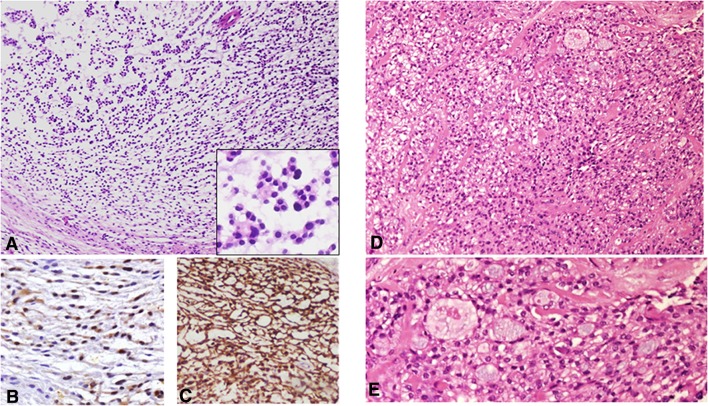
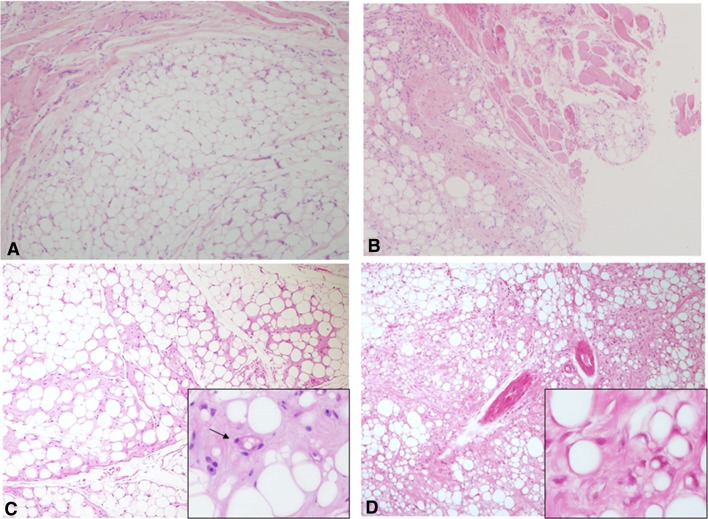
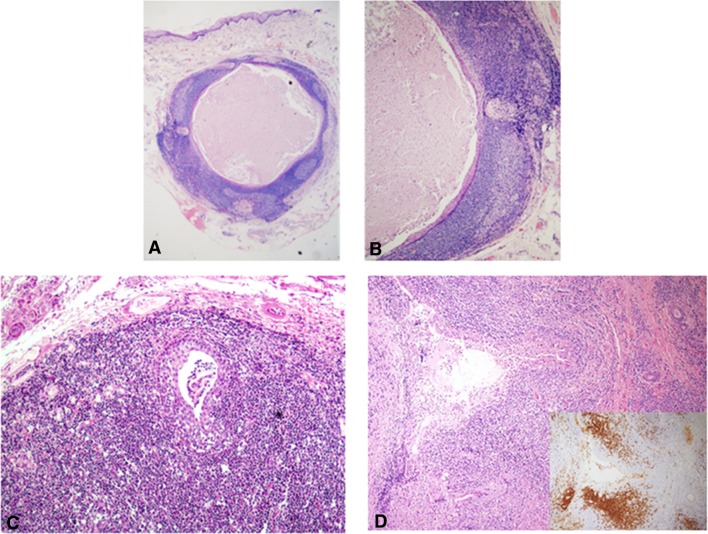
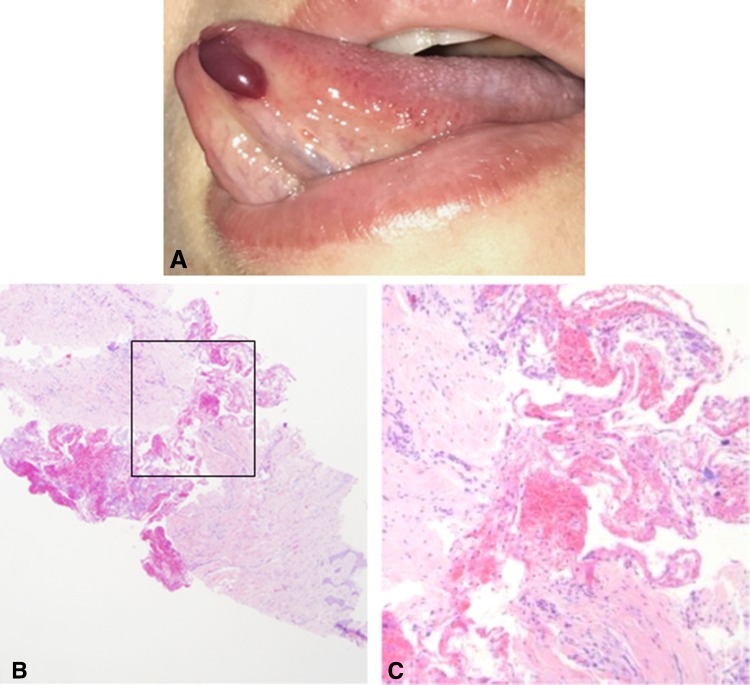
Exophytic lesions of the tongue encompass a diverse spectrum of entities. These are most commonly reactive, arising in response to local trauma but can also be neoplastic of epithelial, mesenchymal or miscellaneous origin. In most cases, the microscopic examination is likely to provide a straightforward diagnosis. However, some cases can still raise microscopic diagnostic dilemmas, such as conditions that mimic malignancies, benign tumors with overlapping features and anecdotal lesions. A series of "lumps and bumps" of the tongue are presented together with suggested clues that can assist in reaching a correct diagnosis, emphasizing the importance of the clinico-pathological correlations.
Keywords: Adipocytic tumors; Lumps and bumps; Lymphoid-rich lesions; Neural lesion; Pseudoepitheliomatous hyperplasia; Spindle cell tumors; Tongue; Verrucous lesions.
Conflict of interest statement
Conflict of interest
Irit Allon, Marilena Vered declares, Ilana Kaplan declares that they have no conflict of interest.
Research Involving Human Participants and/or Animals
This article does not contain any studies with human participants performed by any of the authors.
Figures
References
-
- Brad W, Neville DD, Chi AC, Allen CM. Oral and maxillofacial pathology, 4th edn. Elsevier Health Sciences; 2015. p. 34–35, 336–338, 389–391, 473–475, 497–498, 502–503, 512–514.
-
- Angiero F, Berenzi A, Benetti A, Rossi E, Del Sordo R, Sidoni A, Stefani M, Dessy E. Expression of p16, p53 and Ki-67 proteins in the progression of epithelial dysplasia of the oral cavity. Anticancer Res. 2008;28:2535–2539. - PubMed
-
- Zarovnaya E, Black C. Distinguishing pseudoepitheliomatous hyperplasia from squamous cell carcinoma in mucosal biopsy specimens from the head and neck. Arch Pathol Lab Med. 2005;129:e1032-6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
