

The role of autologous stem cell transplantation in patients with nodal peripheral T-cell lymphomas in first complete remission: Report from COMPLETE, a prospective, multicenter cohort study
- PMID: 30694529
- PMCID: PMC8269282
- DOI: 10.1002/cncr.31861
The role of autologous stem cell transplantation in patients with nodal peripheral T-cell lymphomas in first complete remission: Report from COMPLETE, a prospective, multicenter cohort study
Erratum in
-
Erratum.Cancer. 2019 Nov 1;125(21):3893. doi: 10.1002/cncr.32467. Epub 2019 Aug 14. Cancer. 2019. PMID: 31603547 No abstract available.
Abstract
Background: The role of autologous stem cell transplantation (ASCT) in the first complete remission (CR1) of peripheral T-cell lymphomas (PTCLs) is not well defined. This study analyzed the impact of ASCT on the clinical outcomes of patients with newly diagnosed PTCL in CR1.
Methods: Patients with newly diagnosed, histologically confirmed, aggressive PTCL were prospectively enrolled into the Comprehensive Oncology Measures for Peripheral T-Cell Lymphoma Treatment (COMPLETE) study, and those in CR1 were included in this analysis.
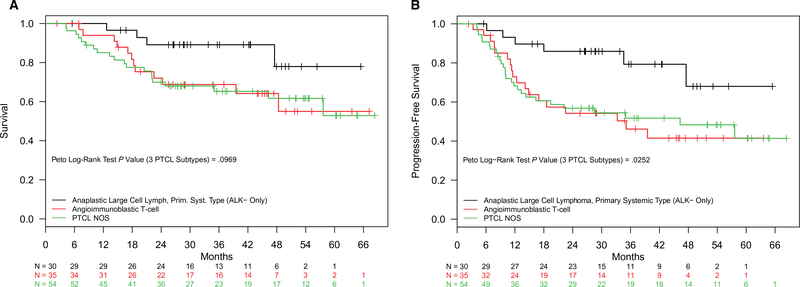
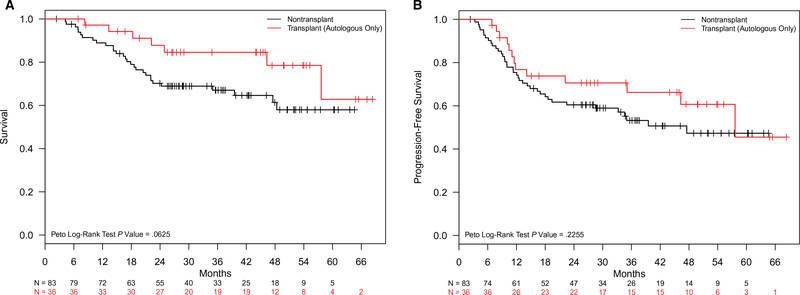
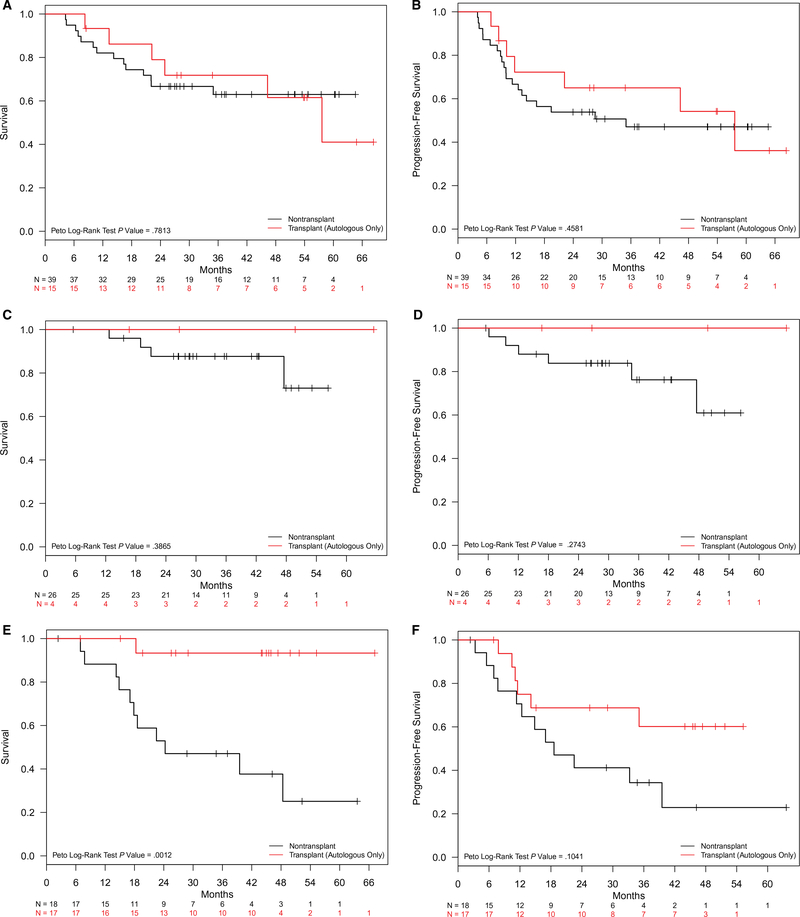
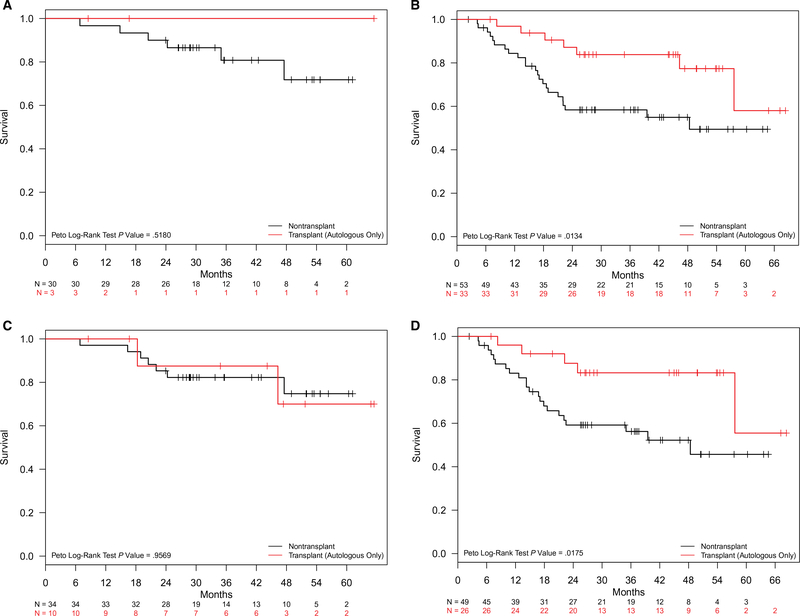
Results: Two hundred thirteen patients with PTCL achieved CR1, and 119 patients with nodal PTCL, defined as anaplastic lymphoma kinase-negative anaplastic large cell lymphoma, angioimmunoblastic T-cell lymphoma (AITL), or PTCL not otherwise specified, were identified. Eighty-three patients did not undergo ASCT, whereas 36 underwent consolidative ASCT in CR1. At the median follow-up of 2.8 years, the median overall survival was not reached for the entire cohort of patients who underwent ASCT, whereas it was 57.6 months for those not receiving ASCT (P = .06). ASCT was associated with superior survival for patients with advanced-stage disease or intermediate-to-high International Prognostic Index scores. ASCT significantly improved overall and progression-free survival for patients with AITL but not for patients with other PTCL subtypes. In a multivariable analysis, ASCT was independently associated with improved survival (hazard ratio, 0.37; 95% confidence interval, 0.15-0.89).
Conclusions: This is the first large prospective cohort study directly comparing the survival outcomes of patients with nodal PTCL in CR1 with or without consolidative ASCT. ASCT may provide a benefit in specific clinical scenarios, but the broader applicability of this strategy should be determined in prospective, randomized trials. These results provide a platform for designing future studies of previously untreated PTCL.
Keywords: anaplastic lymphoma kinase (ALK)-negative anaplastic large cell lymphoma; angioimmunoblastic T-cell lymphoma (AITL); autologous stem cell transplant; first complete remission; nodal peripheral T-cell lymphoma; peripheral T-cell lymphoma (PTCL) not otherwise specified (NOS).
© 2019 American Cancer Society.
Figures
References
-
- Vose JM. Peripheral T-cell non-Hodgkin’s lymphoma. Hematol Oncol Clin North Am. 2008;22:997–1005. - PubMed
-
- Hapgood G, Savage KJ. The biology and management of systemic anaplastic large cell lymphoma. Blood. 2015;126:17–25. - PubMed
-
- Savage KJ. Peripheral T-cell lymphomas. Blood Rev. 2007;21:201–216. - PubMed
-
- Corradini P, Tarella C, Zallio F, et al. Long-term follow-up of patients with peripheral T-cell lymphomas treated up-front with high-dose chemotherapy followed by autologous stem cell transplantation. Leukemia. 2006;20:1533–1538. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
