

A randomized study of solriamfetol for excessive sleepiness in narcolepsy
- PMID: 30694576
- PMCID: PMC6593450
- DOI: 10.1002/ana.25423
A randomized study of solriamfetol for excessive sleepiness in narcolepsy
Erratum in
-
Corrigendum: A Randomized Study of Solriamfetol for Excessive Sleepiness in Narcolepsy.Ann Neurol. 2020 Jan;87(1):157. doi: 10.1002/ana.25632. Epub 2019 Nov 14. Ann Neurol. 2020. PMID: 31833595 Free PMC article. No abstract available.
Abstract
Objective: Solriamfetol (JZP-110) is a selective dopamine and norepinephrine reuptake inhibitor with wake-promoting effects. This phase 3 study (NCT02348593) evaluated the safety and efficacy of solriamfetol in narcolepsy.
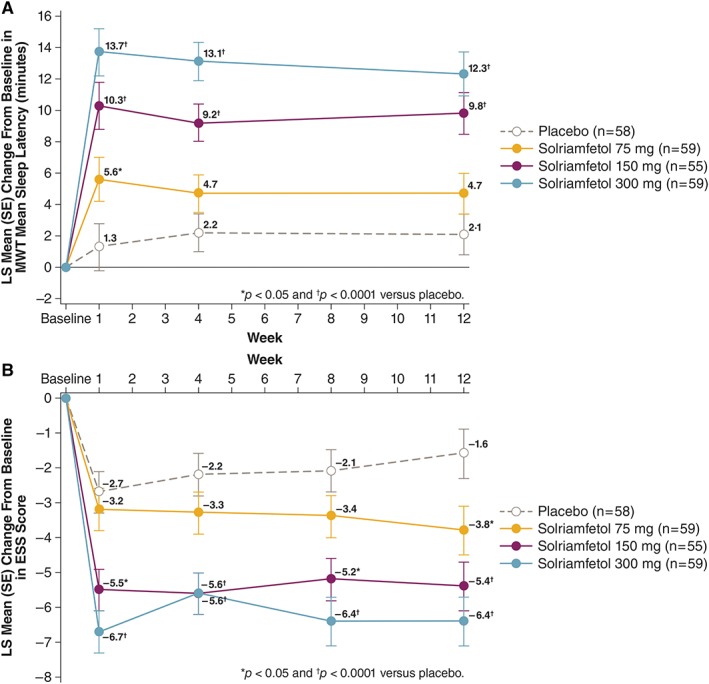
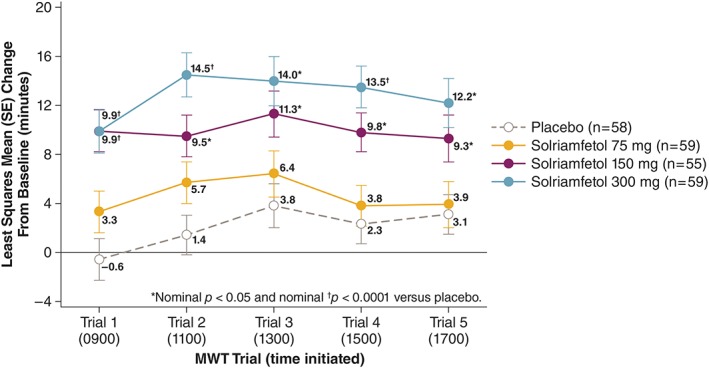
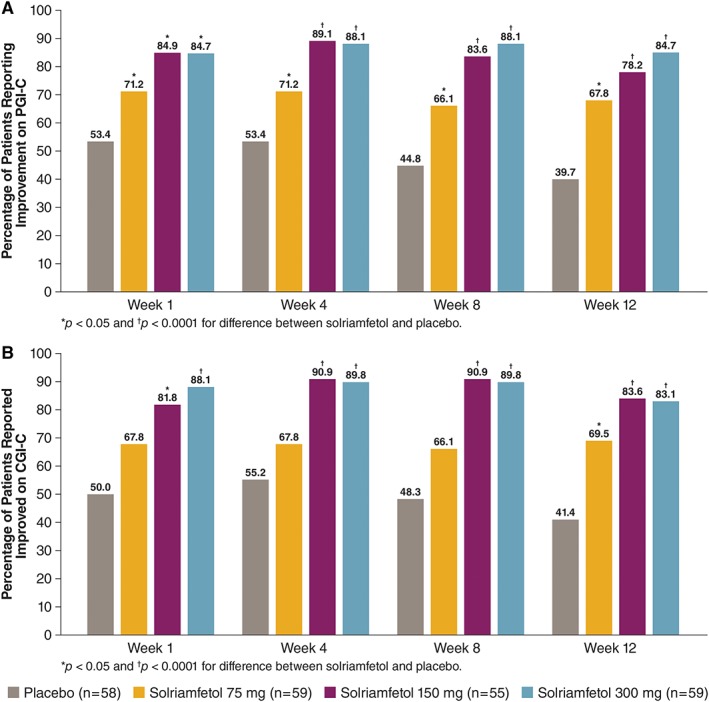
Methods: Patients with narcolepsy with mean sleep latency <25 minutes on the Maintenance of Wakefulness Test (MWT), Epworth Sleepiness Scale (ESS) score ≥10, and usual nightly sleep ≥6 hours were randomized to solriamfetol 75, 150, or 300 mg, or placebo for 12 weeks. Coprimary endpoints were change from baseline to week 12 in MWT and ESS. Improvement on the Patient Global Impression of Change (PGI-C) was the key secondary endpoint.
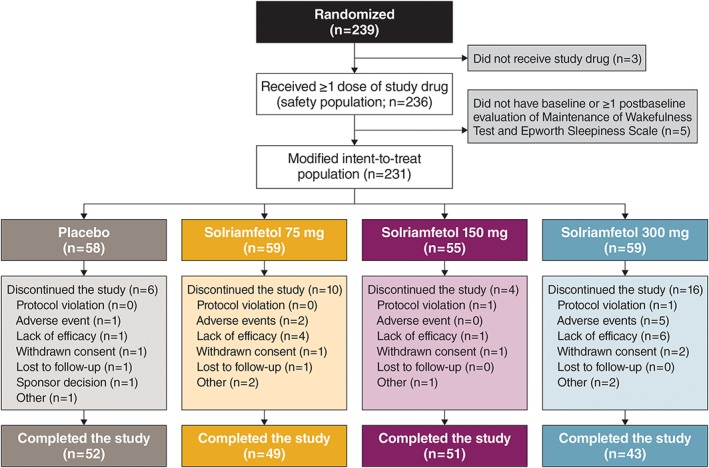
Results: Safety and modified intention-to-treat populations included 236 and 231 patients, respectively. Solriamfetol 300 and 150 mg were positive on both coprimary endpoints. Least squares mean (standard error [SE]) changes from baseline were 12.3 (SE = 1.4) and 9.8 (SE = 1.3) minutes for solriamfetol 300 and 150 mg on the MWT, respectively, versus 2.1 (SE = 1.3) minutes for placebo, and -6.4 (SE = 0.7) for 300 mg and -5.4 (SE = 0.7) for 150 mg on the ESS versus -1.6 (SE = 0.7) for placebo (all p < 0.0001). At week 12, higher percentages of patients treated with solriamfetol 150 mg (78.2%) and 300 mg (84.7%) reported PGI-C improvement relative to placebo (39.7%; both p < 0.0001). Adverse events ≥5% across all solriamfetol doses included headache (21.5%), nausea (10.7%), decreased appetite (10.7%), nasopharyngitis (9.0%), dry mouth (7.3%), and anxiety (5.1%).
Interpretation: Solriamfetol has the potential to be an important therapeutic option for the treatment of impaired wakefulness and excessive sleepiness in patients with narcolepsy. ANN NEUROL 2019;85:359-370.
© 2019 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Conflict of interest statement
In 2014, Jazz Pharmaceuticals acquired a license to develop and commercialize solriamfetol from Aerial Biopharma. Jazz Pharmaceuticals has worldwide development, manufacturing, and commercialization rights to solriamfetol, excluding certain jurisdictions in Asia. SK Biopharmaceuticals, the discoverer of the compound (also known as SKL‐N05), maintains rights in 12 Asian markets, including Korea, China, and Japan. Under the authors’ specific direction on content, organization, and interpretation of the data, E. Jay Bienen, PhD, of the Curry Rockefeller Group (CRG) provided medical writing assistance to the authors, including formatting, proofreading, copyediting, and fact checking, and is hereby acknowledged consistent with International Committee of Medical Journal Editors guidelines. Additional editorial assistance in formatting, proofreading, copyediting, and fact checking was also provided by CRG. The authors had full editorial control of the manuscript and provided their final approval of all content. Jazz Pharmaceuticals provided funding to CRG for editorial support. The following authors disclosed financial relationships with Jazz Pharmaceuticals. M.J.T. has received research/grant support and consultancy and speakers’ bureau fees from Jazz Pharmaceuticals. C.S. has served on the speakers’ bureau for Jazz Pharmaceuticals. H.E. has received research funding and consultancy, honoraria, and/or personal fees from Jazz Pharmaceuticals. G.P. has participated on an advisory board for Jazz Pharmaceuticals. Y.D. has received consultancy fees and/or honoraria and has been a speakers’ bureau member and/or an advisory board participant for Jazz Pharmaceuticals. D.C., L.P.C., and Y.L. are employees of Jazz Pharmaceuticals who, in the course of this employment, have received stock options exercisable for, and other stock awards of, ordinary shares of Jazz Pharmaceuticals. L.P.C. and Y.L. also have a patent pending. J.B. is a part‐time employee of Jazz Pharmaceuticals and shareholder of Jazz Pharmaceuticals. H.W. is a former employee of Jazz Pharmaceuticals. This clinical research was funded by Jazz Pharmaceuticals (the sponsor), which also took a leadership role in designing the study. All of the authors, including authors from Jazz Pharmaceuticals, assisted in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication. G.M. and B.C.C. report no conflicts of interest for the present study.
Figures
References
-
- Dauvilliers Y, Arnulf I, Mignot E. Narcolepsy with cataplexy. Lancet 2007;369:499–511. - PubMed
-
- Thorpy MJ, Dauvilliers Y. Clinical and practical considerations in the pharmacologic management of narcolepsy. Sleep Med 2015;16:9–18. - PubMed
-
- Erman M, Emsellem H, Black J, et al. Correlation between the Epworth Sleepiness Scale and the Maintenance of Wakefulness Test in patients with narcolepsy participating in two clinical trials of sodium oxybate. Sleep Med 2017;38:92–95. - PubMed
-
- Dodel R, Peter H, Spottke A, et al. Health‐related quality of life in patients with narcolepsy. Sleep Med 2007;8:733–741. - PubMed
-
- Ingravallo F, Gnucci V, Pizza F, et al. The burden of narcolepsy with cataplexy: how disease history and clinical features influence socio‐economic outcomes. Sleep Med 2012;13:1293–1300. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
