

Intensivists in U.S. Acute Care Hospitals
- PMID: 30694817
- PMCID: PMC8183575
- DOI: 10.1097/CCM.0000000000003615
Intensivists in U.S. Acute Care Hospitals
Abstract
Objectives: To determine the total numbers of privileged and full-time equivalent intensivists in acute care hospitals with intensivists and compare the characteristics of hospitals with and without intensivists.
Design: Retrospective analysis of the American Hospital Association Annual Survey Database (Fiscal Year 2015).
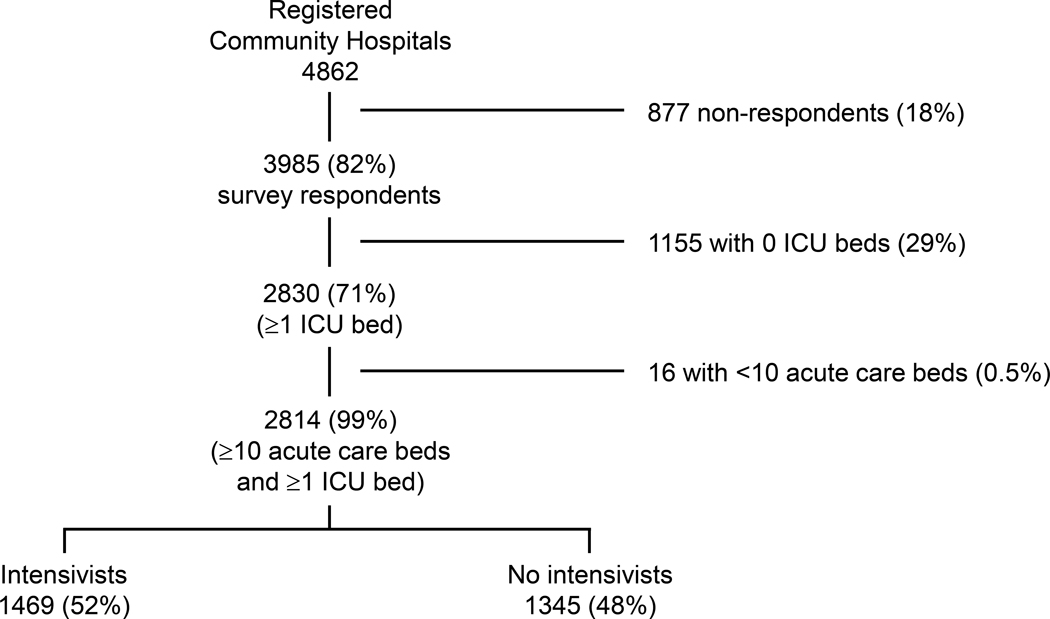
Setting: Two-thousand eight-hundred fourteen acute care hospitals with ICU beds.
Patients: None.
Interventions: None.
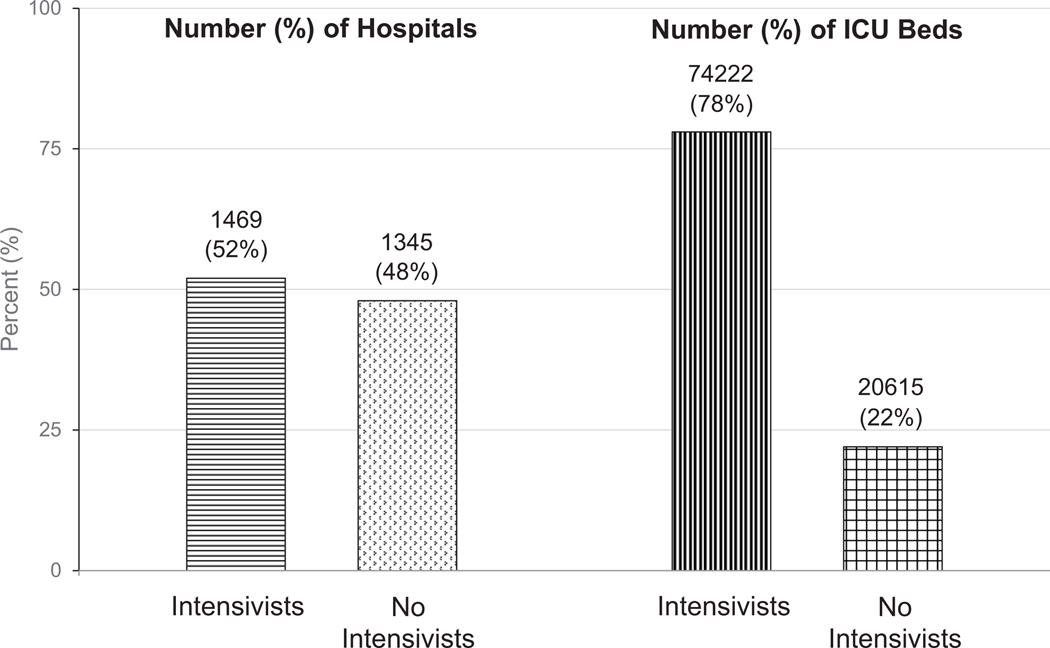
Measurements and main results: Of the 2,814 acute care hospitals studied, 1,469 (52%) had intensivists and 1,345 (48%) had no intensivists. There were 28,808 privileged and 19,996 full-time equivalent intensivists in the 1,469 hospitals with intensivists. In these hospitals, the median (25-75th percentile) numbers of privileged and full-time equivalent intensivists were 11 (5-24) and 7 (2-17), respectively. Compared with hospitals without intensivists, hospitals with privileged intensivists were primarily located in metropolitan areas (91% vs 50%; p < 0.001) and at the aggregate level had nearly thrice the number of hospital beds (403,522 [75%] vs 137,146 [25%]), 3.6 times the number of ICU beds (74,222 [78%] vs 20,615 [22%]), and almost twice as many ICUs (3,383 [65%] vs 1,846 [35%]). At the hospital level, hospitals with privileged intensivists had significantly more hospital beds (median, 213 vs 68; p < 0.0001), ICU beds (median, 32 vs 8; p < 0.0001), a higher ratio of ICU to hospital beds (15.6% vs 12.6%; p < 0.0001), and a higher number of ICUs per hospital (2 vs 1; p < 0.0001) than hospitals without intensivists.
Conclusions: Analyzing the intensivist section of the American Hospital Association Annual Survey database is a novel approach to estimating the numbers of privileged and full-time equivalent intensivists in acute care hospitals with ICU beds in the United States. This methodology opens the door to an enhanced understanding of the current supply and distribution of intensivists as well as future research into the intensivist workforce.
Conflict of interest statement
Figures
Comment in
-
Is There an ICU Doctor in the House?Crit Care Med. 2019 Apr;47(4):604-605. doi: 10.1097/CCM.0000000000003677. Crit Care Med. 2019. PMID: 30882430 Free PMC article. No abstract available.
References
-
- Our patients, Ourselves: Health Care for an Aging Population. A Report of the Dartmouth Atlas Project. 2016. The Dartmouth Institute for Health Policy & Clinical Practice. Available at: http://www.dartmouthatlas.org/downloads/reports/Our_Parents_Ourselves_02.... Accessed May 15, 2018 - PubMed
-
- Godel P, Shimabukuro-Vornhagen A, von Bergwelt-Baildon M. Understanding cytokine release syndrome. Intensive Care Med 2018. March;44(3):371–3. - PubMed
-
- Gooch RA, Kahn JM. ICU Bed Supply, Utilization, and Health Care Spending: An Example of Demand Elasticity. JAMA 2014. January 9;311(6):567–8. - PubMed
-
- Nguyen YL, Wunsch H, Angus DC. Critical care: the impact of organization and management on outcomes. Curr Opin Crit Care 2010. October;16(5):487–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
