

Multicomponent non-pharmacological intervention to prevent delirium for hospitalised people with advanced cancer: study protocol for a phase II cluster randomised controlled trial
- PMID: 30696686
- PMCID: PMC6352777
- DOI: 10.1136/bmjopen-2018-026177
Multicomponent non-pharmacological intervention to prevent delirium for hospitalised people with advanced cancer: study protocol for a phase II cluster randomised controlled trial
Abstract
Introduction: Delirium is a significant medical complication for hospitalised patients. Up to one-third of delirium episodes are preventable in older inpatients through non-pharmacological strategies that support essential human needs, such as physical and cognitive activity, sleep, hydration, vision and hearing. We hypothesised that a multicomponent intervention similarly may decrease delirium incidence, and/or its duration and severity, in inpatients with advanced cancer. Prior to a phase III trial, we aimed to determine if a multicomponent non-pharmacological delirium prevention intervention is feasible and acceptable for this specific inpatient group.
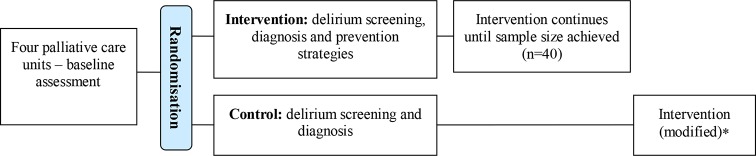
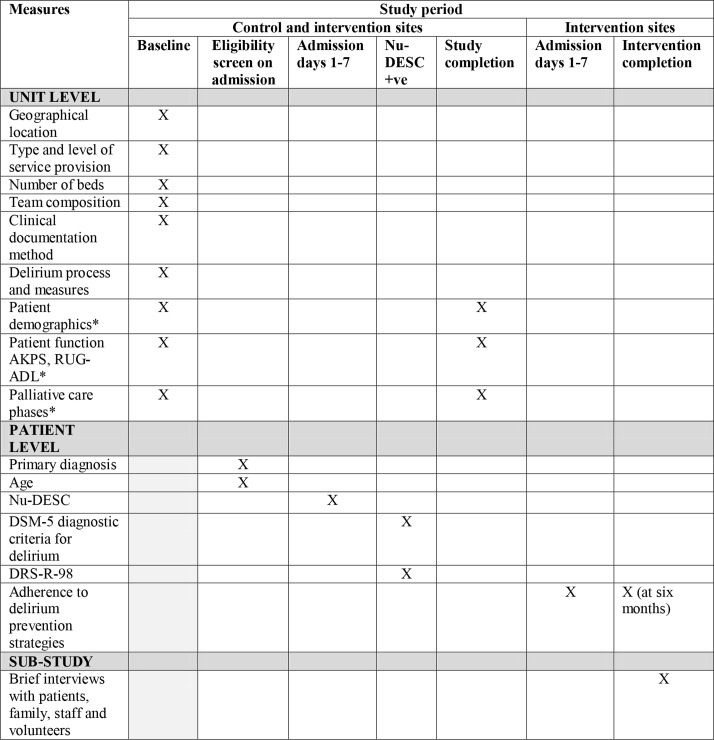
Methods and analysis: The study is a phase II cluster randomised wait-listed controlled trial involving inpatients with advanced cancer at four Australian palliative care inpatient units. Intervention sites will introduce delirium screening, diagnostic assessment and a multicomponent delirium prevention intervention with six domains of care: preserving natural sleep; maintaining optimal vision and hearing; optimising hydration; promoting communication, orientation and cognition; optimising mobility; and promoting family partnership. Interdisciplinary teams will tailor intervention delivery to each site and to patient need. Control sites will first introduce only delirium screening and diagnosis, later implementing the intervention, modified according to initial results. The primary outcome is adherence to the intervention during the first seven days of admission, measured for 40 consecutively admitted eligible patients. Secondary outcomes relate to fidelity and feasibility, acceptability and sustainability of the study intervention, processes and measures in this patient population, using quantitative and qualitative measures. Delirium incidence and severity will be measured to inform power calculations for a future phase III trial.
Ethics and dissemination: Ethical approval was obtained for all four sites. Trial results, qualitative substudy findings and implementation of the intervention will be submitted for publication in peer-reviewed journals, and reported at conferences, to study sites and key peak bodies.
Trial registration number: ACTRN12617001070325; Pre-results.
Keywords: clinical trial; delirium; neoplasms; non-pharmacological; palliative care; prevention.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Arlington, VA: American Psychiatric Publisher, 2013.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical