

Effect of Estrogen on Musculoskeletal Performance and Injury Risk
- PMID: 30697162
- PMCID: PMC6341375
- DOI: 10.3389/fphys.2018.01834
Effect of Estrogen on Musculoskeletal Performance and Injury Risk
Abstract
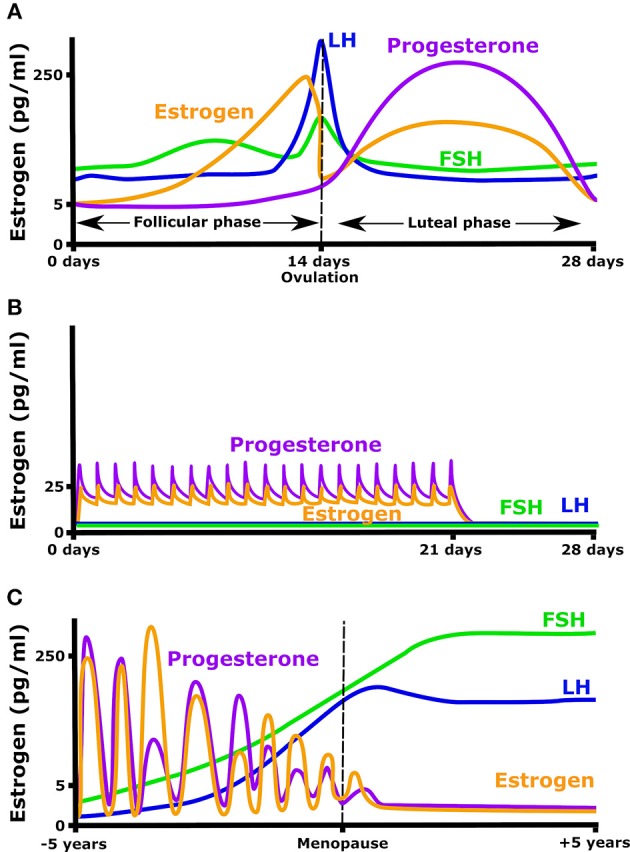
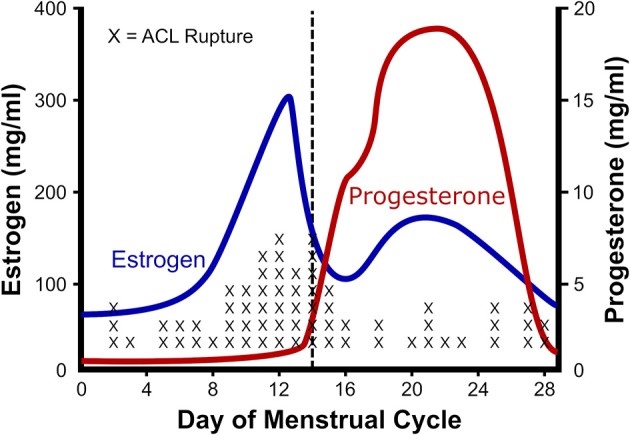
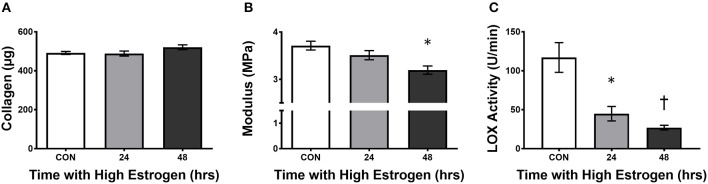
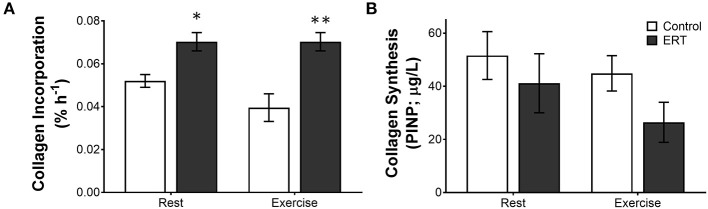
Estrogen has a dramatic effect on musculoskeletal function. Beyond the known relationship between estrogen and bone, it directly affects the structure and function of other musculoskeletal tissues such as muscle, tendon, and ligament. In these other musculoskeletal tissues, estrogen improves muscle mass and strength, and increases the collagen content of connective tissues. However, unlike bone and muscle where estrogen improves function, in tendons and ligaments estrogen decreases stiffness, and this directly affects performance and injury rates. High estrogen levels can decrease power and performance and make women more prone for catastrophic ligament injury. The goal of the current work is to review the research that forms the basis of our understanding how estrogen affects muscle, tendon, and ligament and how hormonal manipulation can be used to optimize performance and promote female participation in an active lifestyle at any age.
Keywords: ACL; estrogen; exercise; injury risk; ligament; muscle; tendon.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical