

Chylothorax secondary to a pleuroperitoneal communication and chylous ascites after pancreatic resection
- PMID: 30697412
- PMCID: PMC6344917
- DOI: 10.1093/jscr/rjy364
Chylothorax secondary to a pleuroperitoneal communication and chylous ascites after pancreatic resection
Abstract
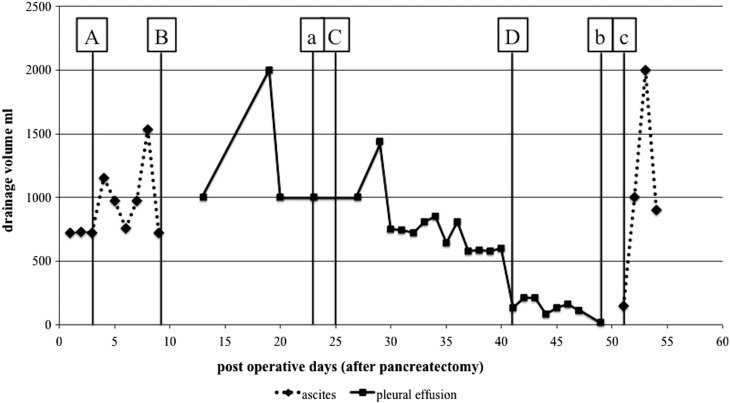
To the best of our knowledge, there have been no previous reports of chylothorax developing after pancreatectomy, although chylous ascites can occur. In patients with a pleuroperitoneal communication, ascitic fluid can flow into the thoracic cavity through a small hole in the diaphragm. A 70-year-old woman underwent total pancreatectomy and was referred to our department for treatment of right chylothorax after removal of her abdominal drainage tubes. An occult pleuroperitoneal communication was detected, and the portion of the diaphragm containing a diaphragmatic fistula was resected using a surgical stapler. After surgery, the chylothorax resolved, but chylous ascites developed. We speculated that this was a rare case of chylous ascites that flowed into the thoracic cavity through a diaphragmatic fistula after a pancreatic resection. When a patient develops chylothorax after an abdominal operation, the combination of a pleuroperitoneal communication and chylous ascites must be considered.
Figures



References
-
- Assumpcao L, Cameron JL, Wolfgang CL, Edil B, Choti MA, Herman JM, et al. . Incidence and management of chyle leaks following pancreatic resection: a high volume single-center institutional experience. J Gastrointest Surg 2008;12:1915–23. - PubMed
-
- Nomoto Y, Suga T, Nakajima K, Sakai H, Osawa G, Ota K, et al. . Acute hydrothorax in continuous ambulatory peritoneal dialysis—a collaborative study of 161 centers. Am J Nephrol 1989;9:363–7. - PubMed
-
- Takagi Y, Sato T, Morio Y, Kumasaka T, Mitani K, Miyamoto H, et al. . A pleuro-peritoneal communication through the diaphragm affected with lymphangioleiomyomatosis. Intern Med 2010;49:439–45. - PubMed
-
- LeVeen HH, Piccone VA, Hutto RB. Management of ascites with hydrothorax. Am J Surg 1984;148:210–3. - PubMed
-
- Zeidan S, Delarue A, Rome A, Roquelaure B. Fibrin glue application in the management of refractory chylous ascites in children. J Pediatr Gastroenterol Nutr 2008;46:478–81. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
