

The role of bone in glenohumeral stability
- PMID: 30697443
- PMCID: PMC6335605
- DOI: 10.1302/2058-5241.3.180028
The role of bone in glenohumeral stability
Abstract
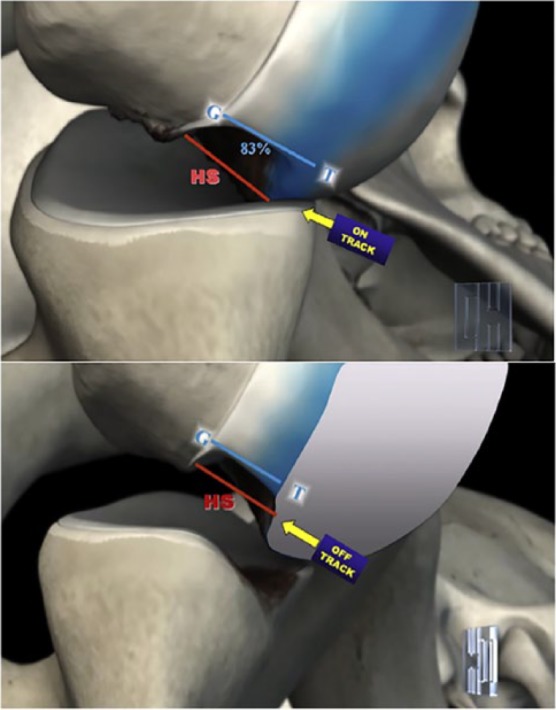
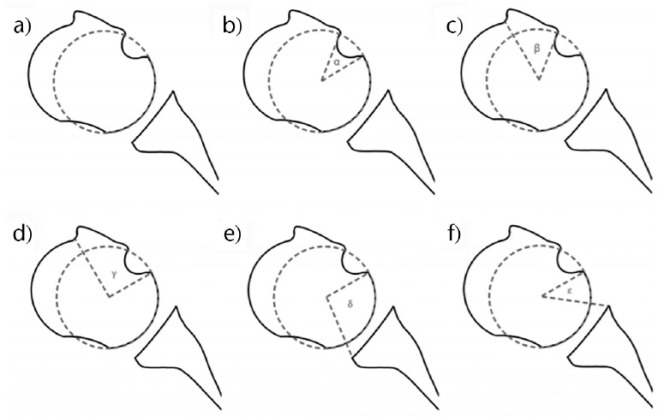
Shoulder stability depends on several factors, either anatomical or functional. Anatomical factors can be further subclassified under soft tissue (shoulder capsule, glenoid rim, glenohumeral ligaments etc) and bony structures (glenoid cavity and humeral head).Normal glenohumeral stability is maintained through factors mostly pertaining to the scapular side: glenoid version, depth and inclination, along with scapular dynamic positioning, can potentially cause decreased stability depending on the direction of said variables in the different planes. No significant factors in normal humeral anatomy seem to play a tangible role in affecting glenohumeral stability.When the glenohumeral joint suffers an episode of acute dislocation, either anterior (more frequent) or posterior, bony lesions often develop on both sides: a compression fracture of the humeral head (or Hill-Sachs lesion) and a bone loss of the glenoid rim. Interaction of such lesions can determine 're-engagement' and recurrence.The concept of 'glenoid track' can help quantify an increased risk of recurrence: when the Hill-Sachs lesion engages the anterior glenoid rim, it is defined as 'off-track'; if it does not, it is an 'on-track' lesion. The position of the Hill-Sachs lesion and the percentage of glenoid bone loss are critical factors in determining the likelihood of recurrent instability and in managing treatment.In terms of posterior glenohumeral instability, the 'gamma angle concept' can help ascertain which lesions are prone to recurrence based on the sum of specific angles and millimetres of posterior glenoid bone loss, in a similar fashion to what happens in anterior shoulder instability. Cite this article: EFORT Open Rev 2018;3:632-640. DOI: 10.1302/2058-5241.3.180028.
Keywords: glenoid track; instability; shoulder.
Conflict of interest statement
ICMJE Conflict of interest statement: G. Di Giacomo declares consultancy for Arthrex; royalties from Springer/Arthrex, activities outside the submitted work.
Figures



References
-
- Kelkar R, Wang VM, Flatow EL, et al. Glenohumeral mechanics: a study of articular geometry, contact, and kinematics. J Shoulder Elbow Surg 2001;10:73–84. - PubMed
-
- Habermeyer P, Schuller U, Wiedemann E. The intra-articular pressure of the shoulder: an experimental study on the role of the glenoid labrum in stabilizing the joint. Arthroscopy 1992;8:166–172. - PubMed
-
- Kumar VP, Balasubramaniam P. The role of atmospheric pressure in stabilising the shoulder: an experimental study. J Bone Joint Surg Br 1985;67-B:719–721. - PubMed
-
- Alexander S, Southgate DF, Bull AM, Wallace AL. The role of negative intraarticular pressure and the long head of biceps tendon on passive stability of the glenohumeral joint. J Shoulder Elbow Surg 2013;22:94–101. - PubMed
-
- Harryman DT, II, Sidles JA, Harris SL, et al. The role of the rotator interval capsule in passivemotion and stability of the shoulder. J Bone Joint Surg Am 1992;74:53–66. - PubMed
LinkOut - more resources
Full Text Sources
