

Association of Surgical Intervention for Adhesive Small-Bowel Obstruction With the Risk of Recurrence
- PMID: 30698610
- PMCID: PMC6537786
- DOI: 10.1001/jamasurg.2018.5248
Association of Surgical Intervention for Adhesive Small-Bowel Obstruction With the Risk of Recurrence
Abstract
Importance: Adhesive small-bowel obstruction (aSBO) is a potentially chronic, recurring surgical illness. Although guidelines suggest trials of nonoperative management, the long-term association of this approach with recurrence is poorly understood.
Objective: To compare the incidence of recurrence of aSBO in patients undergoing operative management at their first admission compared with nonoperative management.
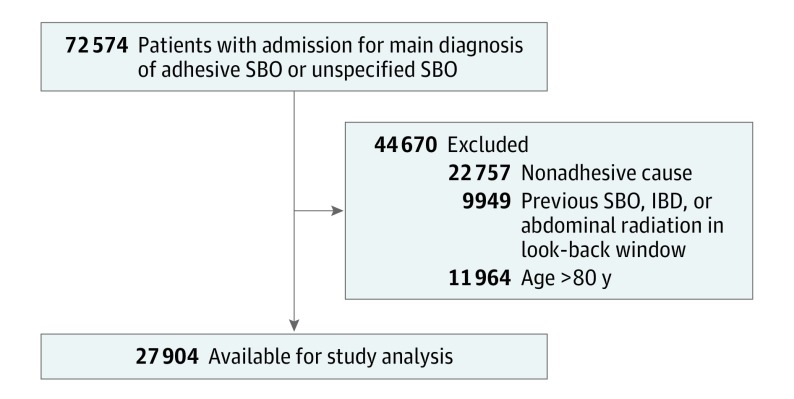
Design, setting, and participants: This longitudinal, propensity-matched, retrospective cohort study used health administrative data for the province of Ontario, Canada, for patients treated from April 1, 2005, through March 31, 2014. The study population included adults aged 18 to 80 years who were admitted for their first episode of aSBO. Patients with nonadhesive causes of SBO were excluded. A total of 27 904 patients were included and matched 1:1 by their propensity to undergo surgery. Factors used to calculate propensity included patient age, sex, comorbidity burden, socioeconomic status, and rurality of home residence. Data were analyzed from September 10, 2017, through October 4, 2018.
Exposures: Operative vs nonoperative management for aSBO.
Main outcomes and measures: The primary outcome was the rate of recurrence of aSBO among those with operative vs nonoperative management. Time-to-event analyses were used to estimate hazard ratios of recurrence while accounting for the competing risk of death.
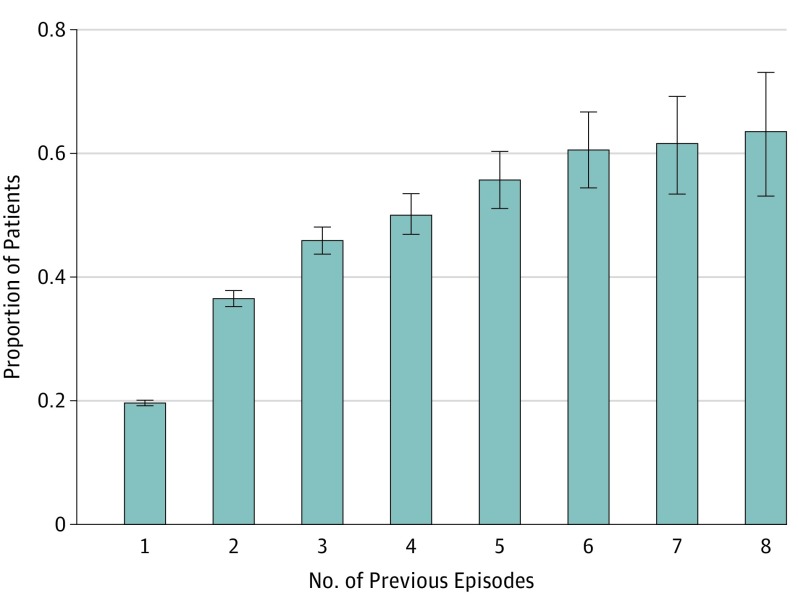
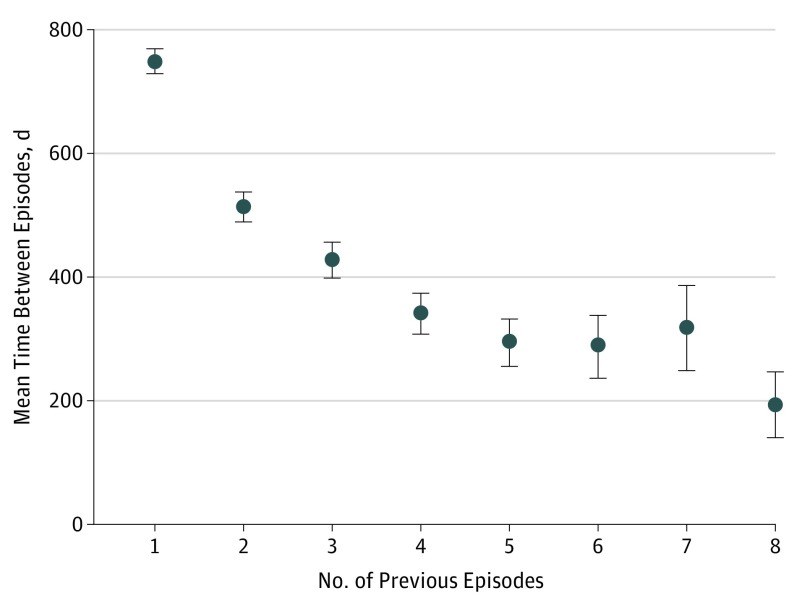
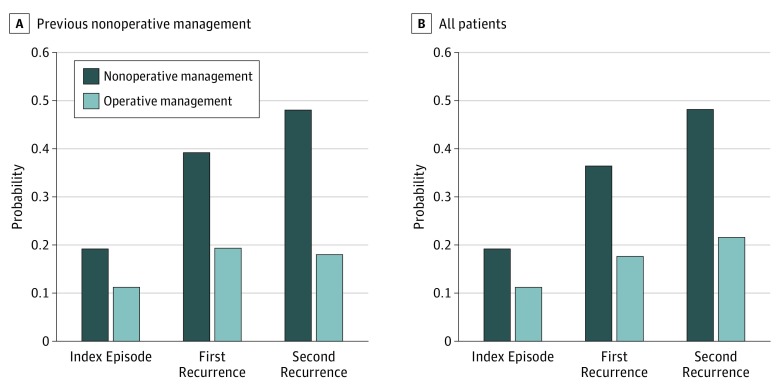
Results: Of 27 904 patients admitted with their first episode of aSBO, 6186 (22.2%) underwent operative management. Mean (SD) patient age was 61.2 (13.6) years, and 51.1% (14 228 of 27 904) were female. Patients undergoing operative management were younger (mean [SD] age, 60.2 [14.3] vs 61.5 [13.4] years) with fewer comorbidities (low burden, 382 [6.2%] vs 912 [4.2%]). After matching, those with operative management had a lower risk of recurrence (13.0% vs 21.3%; hazard ratio, 0.62; 95% CI, 0.56-0.68; P < .001). The 5-year probability of experiencing another recurrence increased with each episode until surgical intervention, at which point the risk of subsequent recurrence decreased by approximately 50%.
Conclusions and relevance: According to this study, operative management of the first episode of aSBO is associated with significantly reduced risk of recurrence. Guidelines advocating trials of nonoperative management for aSBO may assume that surgery increases the risk of recurrence putatively through the formation of additional adhesions. The long-term risk of recurrence of aSBO should be considered in the management of this patient population.
Conflict of interest statement
Figures
Comment in
-
Adhesive Small-Bowel Obstruction-Surgery for All?JAMA Surg. 2019 Nov 1;154(11):1075-1076. doi: 10.1001/jamasurg.2019.2306. JAMA Surg. 2019. PMID: 31339520 No abstract available.
-
Adhesive Small-Bowel Obstruction-Surgery for All?-Reply.JAMA Surg. 2019 Nov 1;154(11):1076-1077. doi: 10.1001/jamasurg.2019.2313. JAMA Surg. 2019. PMID: 31339528 No abstract available.
References
-
- Maung AA, Johnson DC, Piper GL, et al. ; Eastern Association for the Surgery of Trauma . Evaluation and management of small-bowel obstruction: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5)(suppl 4):S362-S369. doi: 10.1097/TA.0b013e31827019de - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
