

Association of the Collagen Signature in the Tumor Microenvironment With Lymph Node Metastasis in Early Gastric Cancer
- PMID: 30698615
- PMCID: PMC6439641
- DOI: 10.1001/jamasurg.2018.5249
Association of the Collagen Signature in the Tumor Microenvironment With Lymph Node Metastasis in Early Gastric Cancer
Abstract
Importance: Lymph node status is the primary determinant in treatment decision making in early gastric cancer (EGC). Current evaluation methods are not adequate for estimating lymph node metastasis (LNM) in EGC.
Objective: To develop and validate a prediction model based on a fully quantitative collagen signature in the tumor microenvironment to estimate the individual risk of LNM in EGC.
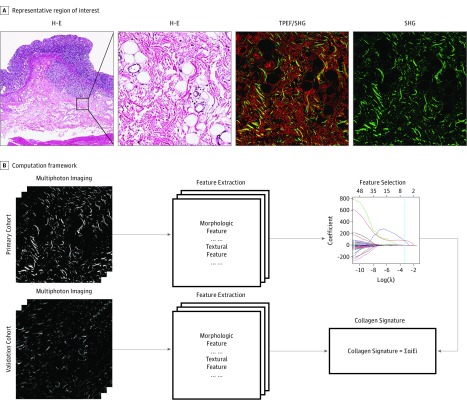
Design, setting, and participants: This retrospective study was conducted from August 1, 2016, to May 10, 2018, at 2 medical centers in China (Nanfang Hospital and Fujian Provincial Hospital). Participants included a primary cohort (n = 232) of consecutive patients with histologically confirmed gastric cancer who underwent radical gastrectomy and received a T1 gastric cancer diagnosis from January 1, 2008, to December 31, 2012. Patients with neoadjuvant radiotherapy, chemotherapy, or chemoradiotherapy were excluded. An additional consecutive cohort (n = 143) who received the same diagnosis from January 1, 2011, to December 31, 2013, was enrolled to provide validation. Baseline clinicopathologic data of each patient were collected. Collagen features were extracted in specimens using multiphoton imaging, and the collagen signature was constructed. An LNM prediction model based on the collagen signature was developed and was internally and externally validated.
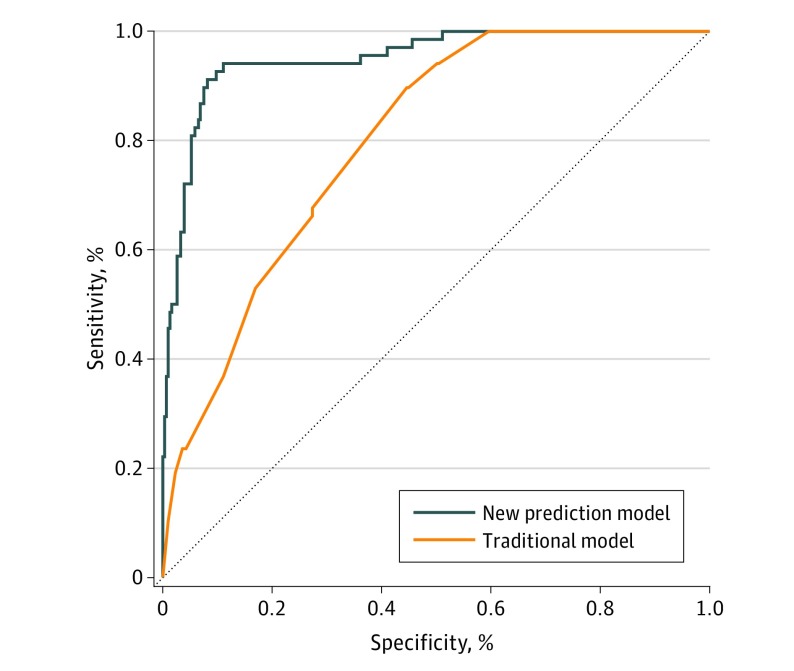
Main outcomes and measures: The area under the receiver operating characteristic curve (AUROC) of the prediction model and decision curve were analyzed for estimating LNM.
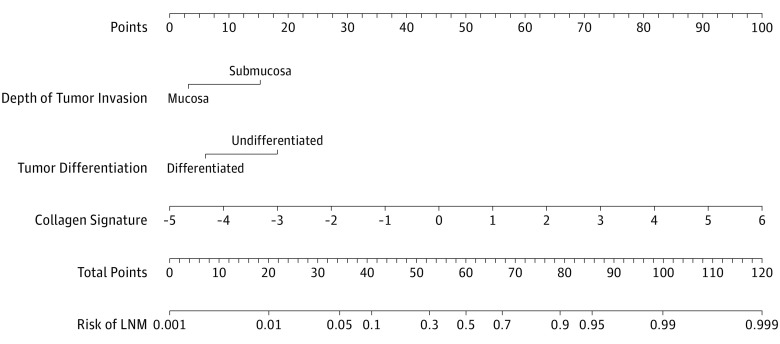
Results: In total, 375 patients were included. The primary cohort comprised 232 consecutive patients, in whom the LNM rate was 16.4% (n = 38; 25 men [65.8%] with a mean [SD] age of 57.82 [10.17] years). The validation cohort consisted of 143 consecutive patients, in whom the LNM rate was 20.9% (n = 30; 20 men [66.7%] with a mean [SD] age of 54.10 [13.19] years). The collagen signature was statistically significantly associated with LNM (odds ratio, 5.470; 95% CI, 3.315-9.026; P < .001). Multivariate analysis revealed that the depth of tumor invasion, tumor differentiation, and the collagen signature were independent predictors of LNM. These 3 predictors were incorporated into the new prediction model, and a nomogram was established. The model showed good discrimination in the primary cohort (AUROC, 0.955; 95% CI, 0.919-0.991) and validation cohort (AUROC, 0.938; 95% CI, 0.897-0.981). An optimal cutoff value was selected in the primary cohort, which had a sensitivity of 86.8%, a specificity of 93.3%, an accuracy of 92.2%, a positive predictive value of 71.7%, and a negative predictive value of 97.3%. The validation cohort had a sensitivity of 90.0%, a specificity of 90.3%, an accuracy of 90.2%, a positive predictive value of 71.1%, and a negative predictive value of 97.1%. Among the 375 patients, a sensitivity of 87.3%, a specificity of 92.1%, an accuracy of 91.2%, a positive predictive value of 72.1%, and a negative predictive value of 96.9% were found.
Conclusions and relevance: This study's findings suggest that the collagen signature in the tumor microenvironment is an independent indicator of LNM in EGC, and the prediction model based on this collagen signature may be useful in treatment decision making for patients with EGC.
Conflict of interest statement
Figures
Comment in
-
Toward More Accurate Understanding of Lymph Node Metastasis Risk in Early Gastric Cancer.JAMA Surg. 2019 Mar 1;154(3):e185250. doi: 10.1001/jamasurg.2018.5250. Epub 2019 Mar 20. JAMA Surg. 2019. PMID: 30698606 No abstract available.
-
Prediction of Lymph Node Metastasis in Early Gastric Cancer by Collagen Signature-Endoscopists' Viewpoint-Reply.JAMA Surg. 2019 Nov 1;154(11):1075. doi: 10.1001/jamasurg.2019.2316. JAMA Surg. 2019. PMID: 31314081 No abstract available.
-
Prediction of Lymph Node Metastasis in Early Gastric Cancer by Collagen Signature-Endoscopists' Viewpoint.JAMA Surg. 2019 Nov 1;154(11):1074-1075. doi: 10.1001/jamasurg.2019.2292. JAMA Surg. 2019. PMID: 31314085 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
