

Patterns of Cause-Specific Mortality Among 2053 Survivors of Retinoblastoma, 1914-2016
- PMID: 30698734
- PMCID: PMC6748807
- DOI: 10.1093/jnci/djy227
Patterns of Cause-Specific Mortality Among 2053 Survivors of Retinoblastoma, 1914-2016
Abstract
Background: Previous studies of hereditary retinoblastoma survivors have reported elevated mortality, particularly for sarcomas, compared with the general population. However, cause-specific mortality patterns for long-term hereditary and nonhereditary retinoblastoma survivors are poorly understood.
Methods: Among 2053 retinoblastoma patients diagnosed during 1914-2006 at two major US treatment centers and followed to 2016, we estimated cumulative mortality, standardized mortality ratios (SMRs), and absolute excess risks (AERs) compared with the US general population.
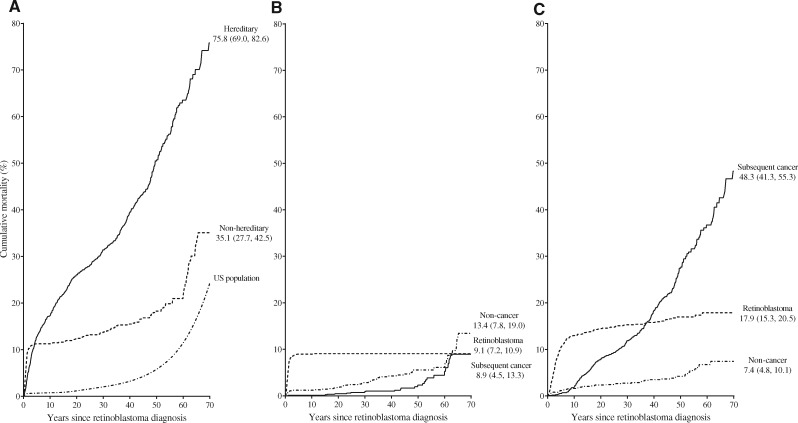
Results: Most deaths occurred in 1129 hereditary retinoblastoma patients (n = 518 deaths, cumulative mortality 70 years after retinoblastoma = 75.8%, 95% CI = 69.0% to 82.6%; SMR = 8.5, 95% CI = 7.7 to 9.2). Of these, 267 were due to subsequent cancers (SMR = 27.4, 95% CI = 24.2 to 30.9; AER = 72.3 deaths/10 000 person-years), for which SMRs were highest 15-29 years after diagnosis (n = 69, SMR = 89.9, 95% CI = 70.0 to 113.8) but remained statistically significantly elevated at 60 and more years (n = 14, SMR = 6.7, 95% CI = 3.6 to 11.2), whereas AERs increased with time (AER<15years = 38.0; AER60+years = 327.5). Increased risk of death due to cancers of pancreas, large intestines, and kidney were noted for the first time. Overall risk of subsequent cancers was greater for those treated with radiotherapy and chemotherapy compared to radiotherapy alone, although patterns varied by organ site. For 924 patients with nonhereditary retinoblastoma, we noted a modestly increased risk of death for subsequent cancers (n = 27, SMR = 1.8, 95% CI = 1.2 to 2.6) possibly due to treatment or misclassification of hereditary status. Risks of noncancer causes of death were not elevated for hereditary or nonhereditary patients.
Conclusion: Hereditary retinoblastoma survivors died mainly from an excess risk of subsequent cancers up to six decades later, highlighting the need to develop long-term clinical management guidelines for hereditary retinoblastoma survivors treated in the past.
Published by Oxford University Press 2019.
Figures
References
-
- Noone AM,, Howlader N, Krapcho M, eds, et al. SEER Cancer Statistics Review, 1975–2015. Bethesda, MD: National Cancer Institute. https://seer.cancer.gov/csr/1975_2015/. Accessed April 2018.
-
- Marees T, Moll AC, Imhof SM, et al. Risk of second malignancies in survivors of retinoblastoma: more than 40 years of follow-up. J Natl Cancer Inst. 2008;10024:1771–1779. - PubMed
-
- Temming P, Arendt M, Viehmann A, et al. Incidence of second cancers after radiotherapy and systemic chemotherapy in heritable retinoblastoma survivors: a report from the German reference center. Pediatr Blood Cancer. 2017;641:71–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
