

Factors affecting mortality among HIV positive patients two years after completing recommended therapy for Cryptococcal meningitis in Uganda
- PMID: 30699151
- PMCID: PMC6353088
- DOI: 10.1371/journal.pone.0210287
Factors affecting mortality among HIV positive patients two years after completing recommended therapy for Cryptococcal meningitis in Uganda
Abstract
Background: Cryptococcal meningitis (CCM) remains a leading cause of mortality amongst HIV infected patients in sub-Saharan Africa. When patients receive recommended therapy, mortality at 10 weeks has been reported to vary between 20 to 36%. However, mortality rate and factors affecting mortality after completing recommended therapy are not well known. We investigated mortality rate, and factors affecting mortality at 2 years among CCM patients following completion of recommended CCM therapy in Uganda.
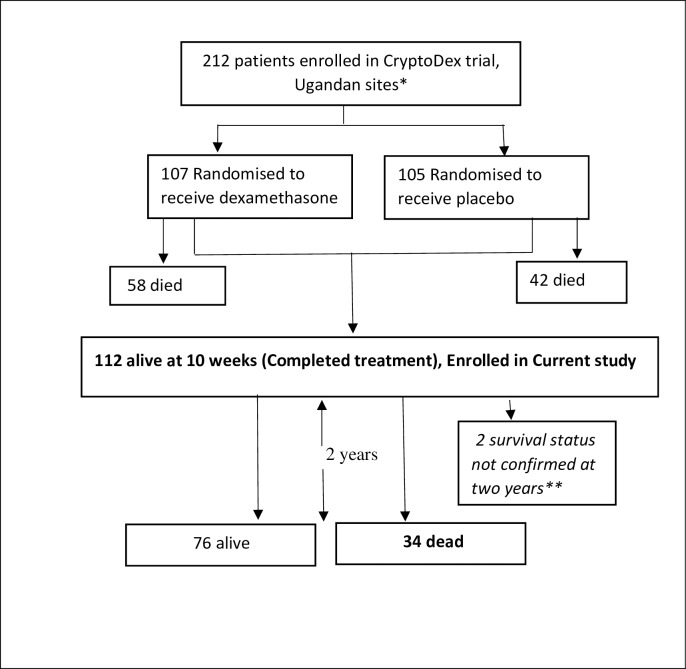
Methods: A retrospective cohort study was conducted among HIV infected patients that had completed 10 weeks of recommended therapy for CCM (2 weeks of intravenous amphotericin B 1mg/kg and 10 weeks of oral Fluconazole 800mg daily) in the CryptoDex trial (ISRCTN59144167) between 2013 and 2015. Survival analysis applying Cox regression was used to determine the mortality rate and factors affecting mortality at 2 years.
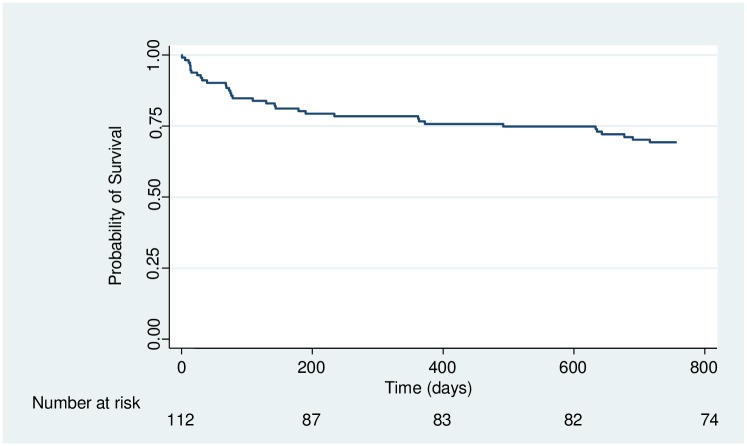
Results: This study followed up 112 participants for 2 years. Mean age (±SD) was 34.9 ± 8, 48 (57.1%) were female and 80 (74.8%) had been on ART for less than 1 year. At 2 years, overall mortality was 30.9% (20 deaths per 100 person-years). Majority of deaths (61.8%) occurred during the first 6 months. In multivariable analysis, mortality was associated with ever being re-admitted since discharge after hospital-based management of CCM (aHR = 13.33, 95% CI: 5.92-30.03), p<0.001; and self-perceived quality of life, with quality of life 50-75% having reduced risk compared to <50% (aHR = 0.21, 95% CI: 0.09-0.5), p<0.001, as well as >75% compared to <50% (HR = 0.29, 95% CI: 0.11-0.81), p = 0.018.
Conclusion: There remains a considerable risk of mortality in the first two years after completion of standard therapy for CCM in resource-limited settings with risk highest during the first 6 months. Maintenance of patient follow up during this period may reduce mortality.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
