

Oral versus Intravenous Antibiotics for Bone and Joint Infection
- PMID: 30699315
- PMCID: PMC6522347
- DOI: 10.1056/NEJMoa1710926
Oral versus Intravenous Antibiotics for Bone and Joint Infection
Abstract
Background: The management of complex orthopedic infections usually includes a prolonged course of intravenous antibiotic agents. We investigated whether oral antibiotic therapy is noninferior to intravenous antibiotic therapy for this indication.
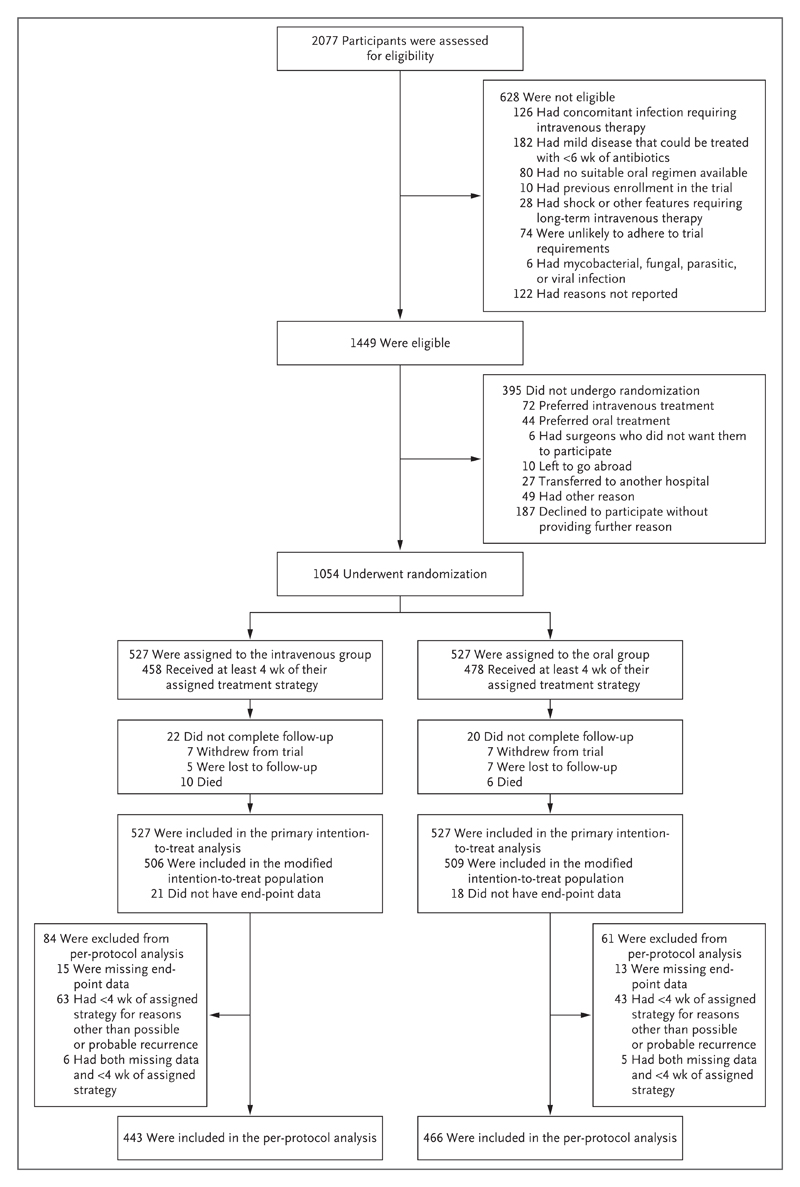
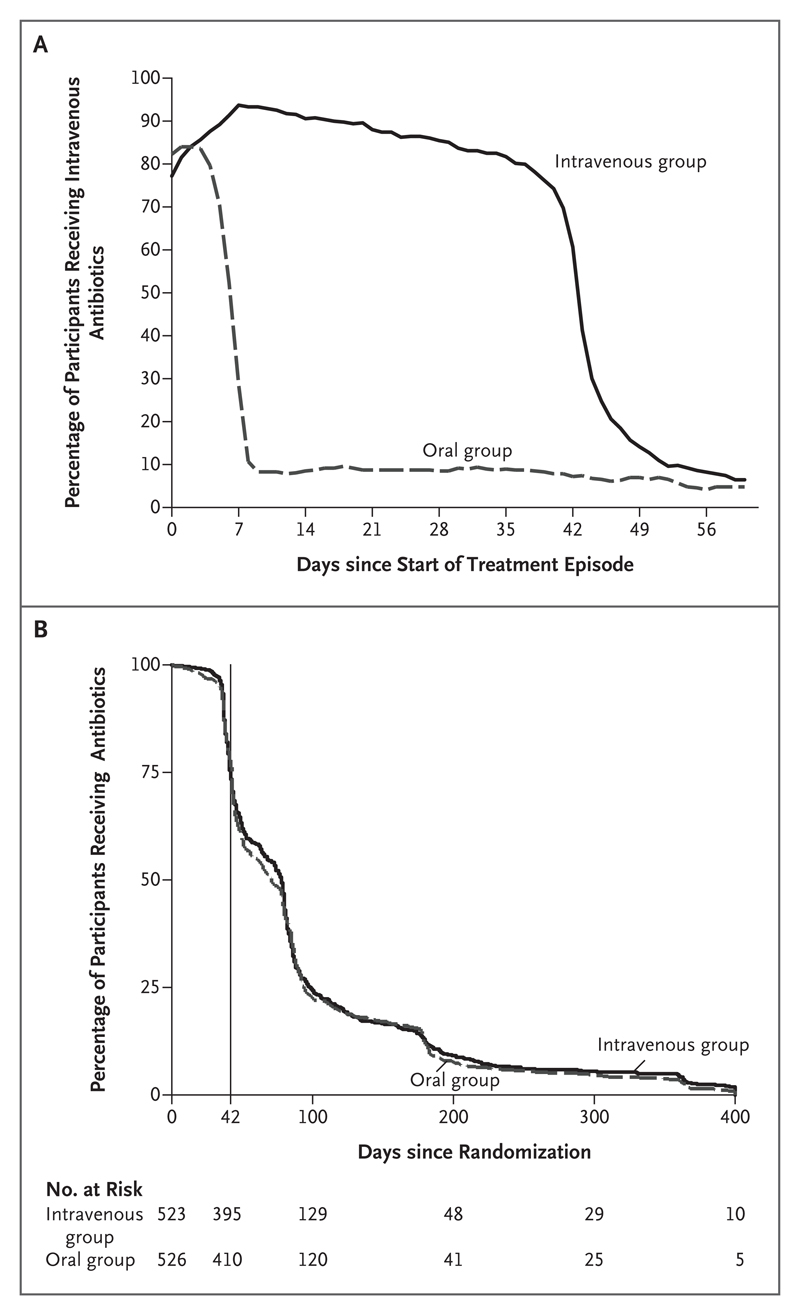
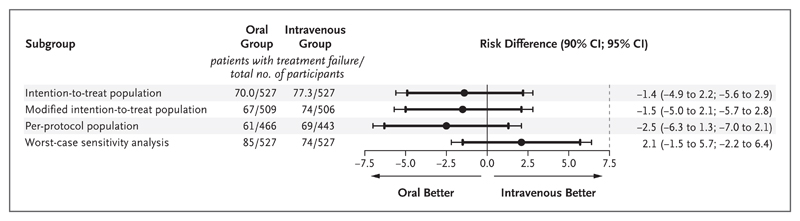
Methods: We enrolled adults who were being treated for bone or joint infection at 26 U.K. centers. Within 7 days after surgery (or, if the infection was being managed without surgery, within 7 days after the start of antibiotic treatment), participants were randomly assigned to receive either intravenous or oral antibiotics to complete the first 6 weeks of therapy. Follow-on oral antibiotics were permitted in both groups. The primary end point was definitive treatment failure within 1 year after randomization. In the analysis of the risk of the primary end point, the noninferiority margin was 7.5 percentage points.
Results: Among the 1054 participants (527 in each group), end-point data were available for 1015 (96.3%). Treatment failure occurred in 74 of 506 participants (14.6%) in the intravenous group and 67 of 509 participants (13.2%) in the oral group. Missing end-point data (39 participants, 3.7%) were imputed. The intention-to-treat analysis showed a difference in the risk of definitive treatment failure (oral group vs. intravenous group) of -1.4 percentage points (90% confidence interval [CI], -4.9 to 2.2; 95% CI, -5.6 to 2.9), indicating noninferiority. Complete-case, per-protocol, and sensitivity analyses supported this result. The between-group difference in the incidence of serious adverse events was not significant (146 of 527 participants [27.7%] in the intravenous group and 138 of 527 [26.2%] in the oral group; P=0.58). Catheter complications, analyzed as a secondary end point, were more common in the intravenous group (9.4% vs. 1.0%).
Conclusions: Oral antibiotic therapy was noninferior to intravenous antibiotic therapy when used during the first 6 weeks for complex orthopedic infection, as assessed by treatment failure at 1 year. (Funded by the National Institute for Health Research; OVIVA Current Controlled Trials number, ISRCTN91566927 .).
Figures
Comment in
-
Partial Oral Therapy for Osteomyelitis and Endocarditis - Is It Time?N Engl J Med. 2019 Jan 31;380(5):487-489. doi: 10.1056/NEJMe1817264. N Engl J Med. 2019. PMID: 30699312 No abstract available.
-
Initial oral antibiotic therapy was noninferior to IV therapy for treatment failure in orthopedic infection at 1 y.Ann Intern Med. 2019 May 21;170(10):JC58. doi: 10.7326/ACPJ201905210-058. Ann Intern Med. 2019. PMID: 31108520 No abstract available.
-
Partial Oral Therapy for Osteomyelitis and Endocarditis.N Engl J Med. 2019 Sep 19;381(12):1182. doi: 10.1056/NEJMc1904725. N Engl J Med. 2019. PMID: 31532971 No abstract available.
-
Partial Oral Therapy for Osteomyelitis and Endocarditis.N Engl J Med. 2019 Sep 19;381(12):1182-1183. doi: 10.1056/NEJMc1904725. N Engl J Med. 2019. PMID: 31532972 No abstract available.
-
Partial Oral Therapy for Osteomyelitis and Endocarditis.N Engl J Med. 2019 Sep 19;381(12):1183. doi: 10.1056/NEJMc1904725. N Engl J Med. 2019. PMID: 31532973 No abstract available.
-
Partial Oral Therapy for Osteomyelitis and Endocarditis.N Engl J Med. 2019 Sep 19;381(12):1183. doi: 10.1056/NEJMc1904725. N Engl J Med. 2019. PMID: 31532974 No abstract available.
-
Partial Oral Therapy for Osteomyelitis and Endocarditis.N Engl J Med. 2019 Sep 19;381(12):1183. doi: 10.1056/NEJMc1904725. N Engl J Med. 2019. PMID: 31532975 No abstract available.
-
The opioid epidemic and intravenous drug-associated endocarditis: A path forward.J Thorac Cardiovasc Surg. 2020 Apr;159(4):1273-1278. doi: 10.1016/j.jtcvs.2019.08.112. Epub 2019 Oct 15. J Thorac Cardiovasc Surg. 2020. PMID: 31627948 No abstract available.
-
Oral antibiotic therapy in diabetic foot osteomyelitis: one small step or a giant leap of faith?Ann Transl Med. 2019 Dec;7(Suppl 8):S266. doi: 10.21037/atm.2019.12.53. Ann Transl Med. 2019. PMID: 32015985 Free PMC article. No abstract available.
References
-
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364:369–79. - PubMed
-
- Zimmerli W, Ochsner PE. Management of infection associated with prosthetic joints. Infection. 2003;31:99–108. - PubMed
-
- Waldvogel FA, Medoff G, Swartz MN. Osteomyelitis: a review of clinical features, therapeutic considerations and unusual aspects. N Engl J Med. 1970;282:198–206. - PubMed