

Glucose Activates Vagal Control of Hyperglycemia and Inflammation in Fasted Mice
- PMID: 30700738
- PMCID: PMC6354016
- DOI: 10.1038/s41598-018-36298-z
Glucose Activates Vagal Control of Hyperglycemia and Inflammation in Fasted Mice
Abstract
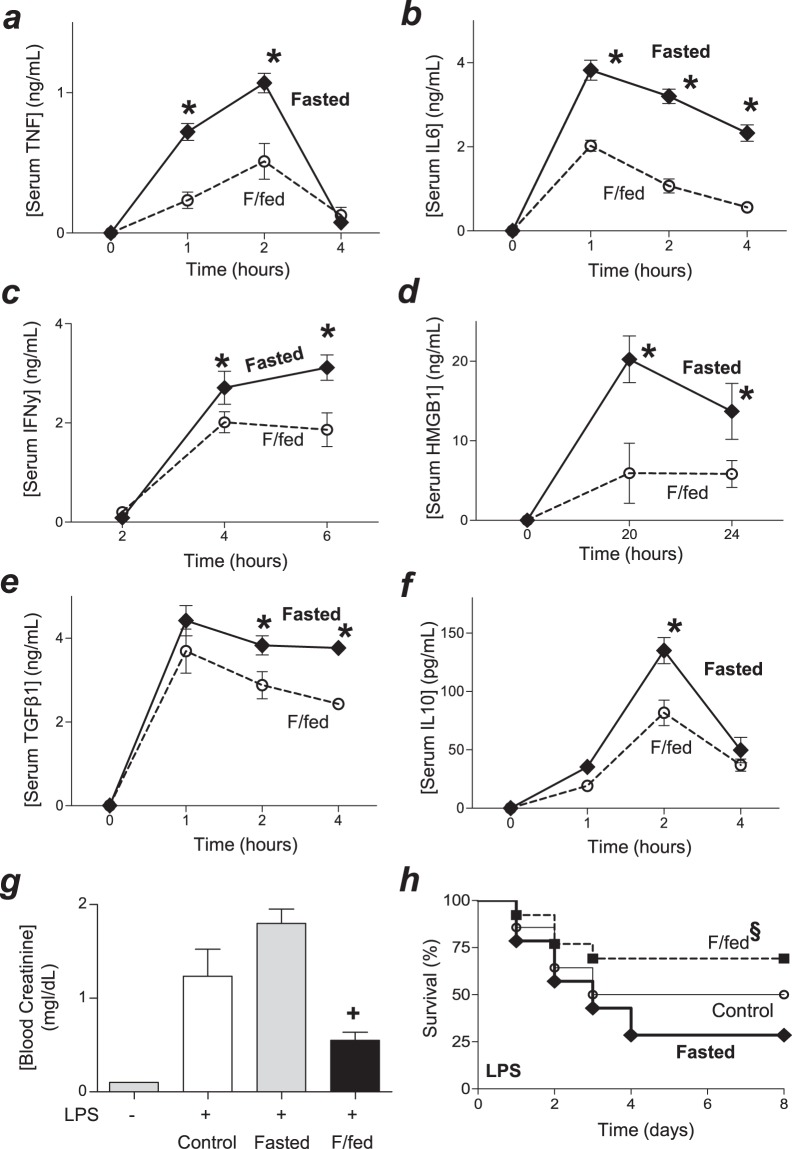
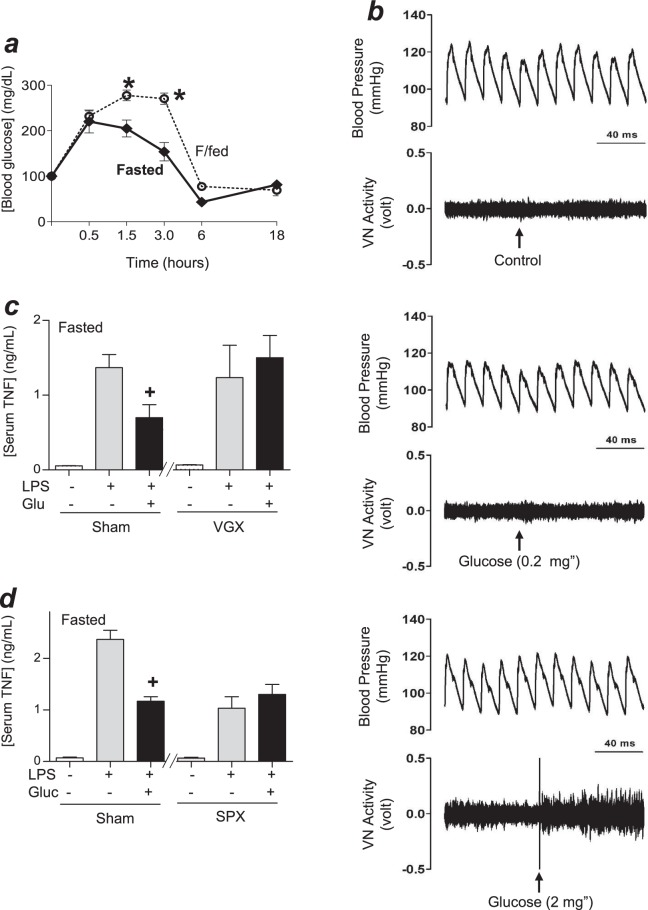
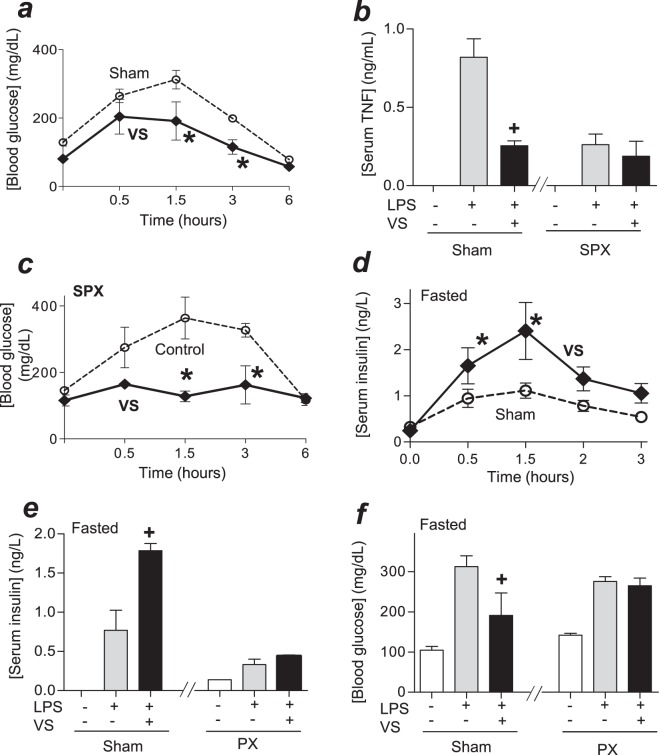
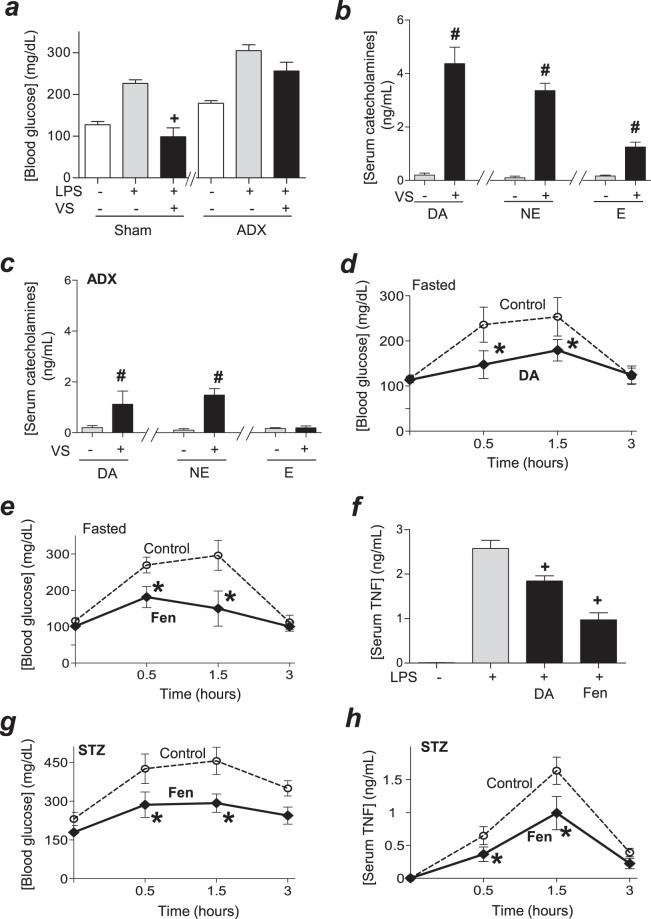
Sepsis is a leading cause of death in hospitalized patients. Many experimental treatments may have failed in clinical trials for sepsis, in part, because they focused on immune responses of healthy animals that did not mimic the metabolic settings of septic patients. Epidemiological studies show an association between metabolic and immune alterations and over 1/3 of septic patients are diabetic, but the mechanism linking these systems is unknown. Here, we report that metabolic fasting increased systemic inflammation and worsened survival in experimental sepsis. Feeding and administration of glucose in fasted mice activated the vagal tone without affecting blood pressure. Vagal stimulation attenuated hyperglycemia and serum TNF levels in sham but only hyperglycemia in splenectomized mice. Vagal stimulation induced the production of dopamine from the adrenal glands. Experimental diabetes increased hyperglycemia and systemic inflammation in experimental sepsis. Fenoldopam, a specific dopaminergic type-1 agonist, attenuated hyperglycemia and systemic inflammation in diabetic endotoxemic mice. These results indicate that glucose activates vagal control of hyperglycemia and inflammation in fasted septic mice via dopamine.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
