

Prenatal diagnosis of fetal intraabdominal extralobar pulmonary sequestration: a 12-year 3-center experience in China
- PMID: 30700771
- PMCID: PMC6353922
- DOI: 10.1038/s41598-018-37268-1
Prenatal diagnosis of fetal intraabdominal extralobar pulmonary sequestration: a 12-year 3-center experience in China
Abstract
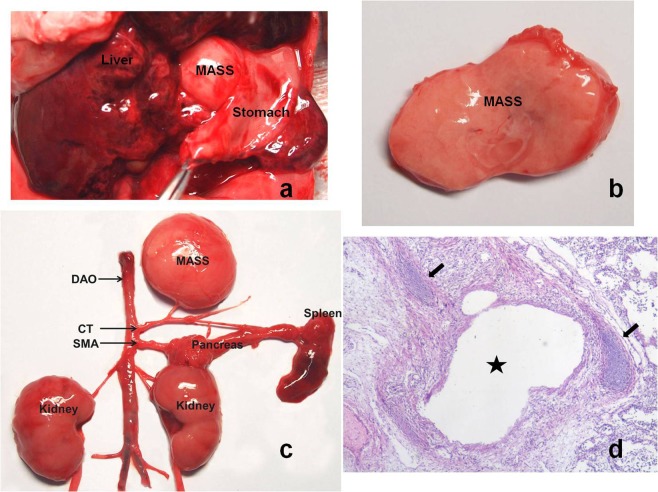
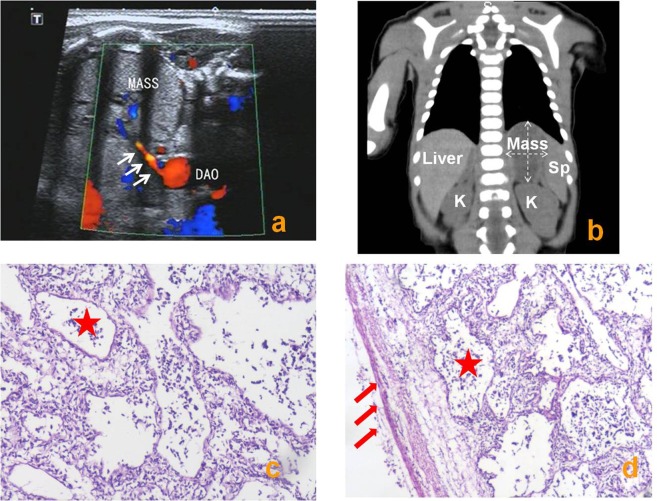
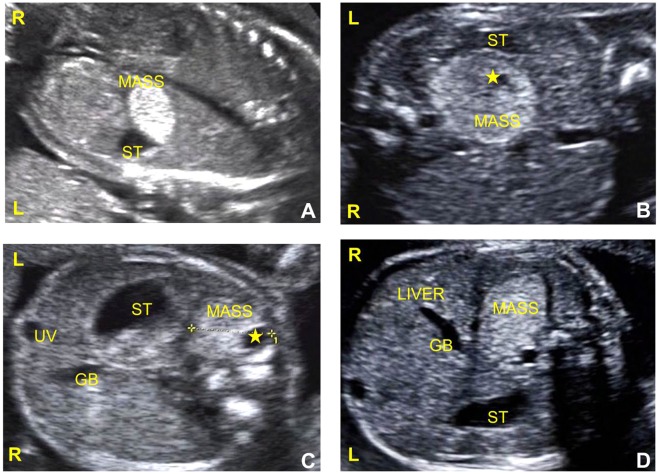
To provide useful information for diagnosing and predicting fetal intraabdominal extralobar pulmonary sequestration (IEPS), a retrospective review of diagnostic approaches was conducted. Ultrasonography was performed serially in 21 fetuses with IEPS from 2005 to 2017. Prenatal sonographic features, treatment, and outcomes of each case were evaluated and collected. These cases of IEPS were also compared to 43 cases previously reported by other researchers from 1986 to 2017. Of the 21 sonographic features, 14 (67%) were hyperechoic, 21 (100%) were well circumscribed, and 17 (81%) depicted a mass that shifted with fetal breaths/hiccups non-synchronized with adjacent organs (sliding sign). Feeding arteries were detected prenatally in 18 patients (86%). The lesion volume was 10.17 ± 4.66 cm3, the congenital cystic adenomatoid malformation volume ratio and cardiothoracic ratio were in normal range. The gestational age at diagnosis, location and echotexture of the lesion, and rate of surgical treatment were similar to previous studies, but with a significantly higher rate of detected feeding arteries (P < 0.01), and associated anomalies (P < 0.01). All infants who underwent surgery after birth had satisfactory outcomes. The sliding sign and feeding artery are essential features of IEPS in prenatal diagnosis.
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Intraabdominal extralobar pulmonary sequestration exhibiting cystic adenomatoid malformation: prenatal diagnosis and characterization of a left suprarenal mass in the newborn.Abdom Imaging. 2001 Jan-Feb;26(1):28-31. doi: 10.1007/s002610000096. Abdom Imaging. 2001. PMID: 11116355
-
Fetal lung lesions: management and outcome.Am J Obstet Gynecol. 1998 Oct;179(4):884-9. doi: 10.1016/s0002-9378(98)70183-8. Am J Obstet Gynecol. 1998. PMID: 9790364
-
Cystic sonographic appearance of extralobar pulmonary sequestration.Pediatr Radiol. 1993;23(8):605-7. doi: 10.1007/BF02014979. Pediatr Radiol. 1993. PMID: 8152876
-
Presumptive intrahepatic congenital cystic adenomatoid malformation.J Ultrasound Med. 2003 May;22(5):531-6. doi: 10.7863/jum.2003.22.5.531. J Ultrasound Med. 2003. PMID: 12751866 Review.
-
Current outcome of antenally diagnosed cystic lung disease.J Pediatr Surg. 2004 Apr;39(4):549-56. doi: 10.1016/j.jpedsurg.2003.12.021. J Pediatr Surg. 2004. PMID: 15065026 Review.
Cited by
-
Epidemiology and prevalence of pulmonary sequestration in Chinese population, 2010-2019.BMC Pulm Med. 2023 Jan 9;23(1):8. doi: 10.1186/s12890-023-02308-8. BMC Pulm Med. 2023. PMID: 36624419 Free PMC article.
References
-
- Cooke CR. Bronchopulmonary sequestration. Respir Care. 2006;51:661–664. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
