

What is a tongue tie? Defining the anatomy of the in-situ lingual frenulum
- PMID: 30701608
- PMCID: PMC6850428
- DOI: 10.1002/ca.23343
What is a tongue tie? Defining the anatomy of the in-situ lingual frenulum
Abstract
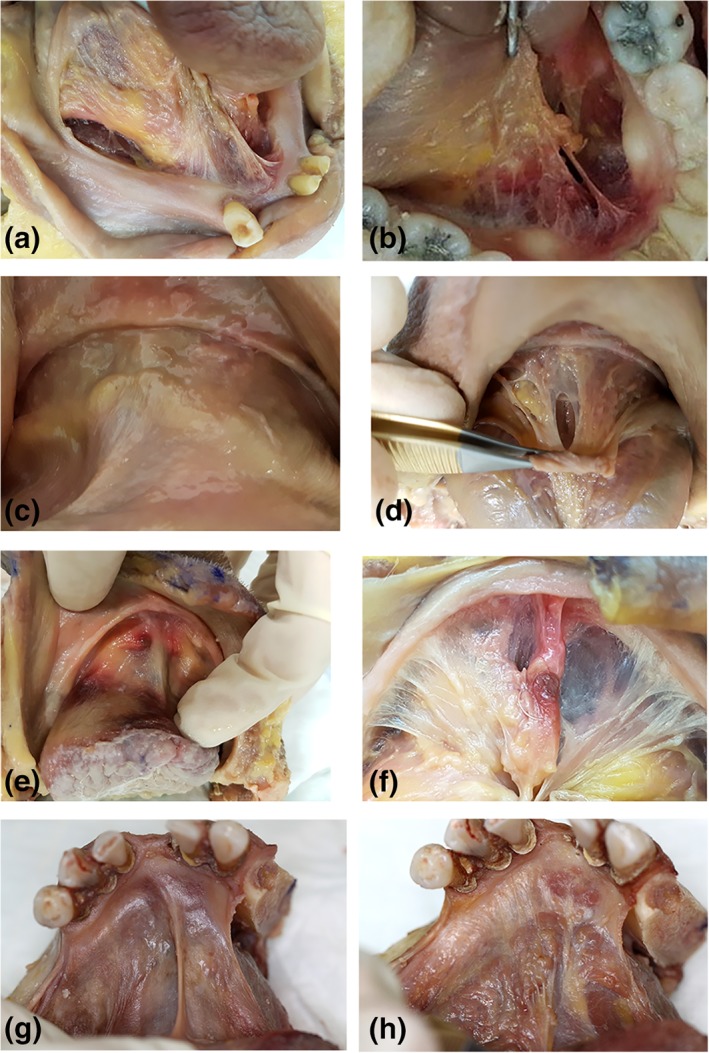
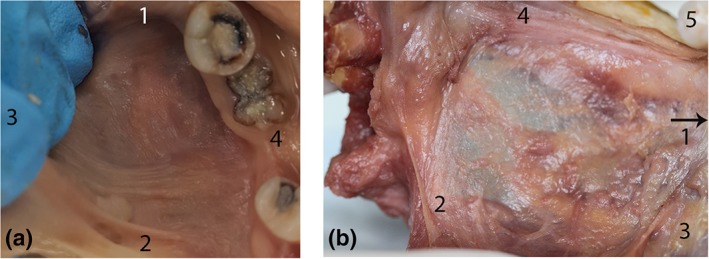
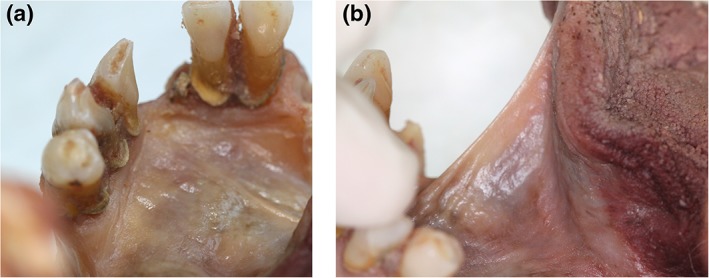
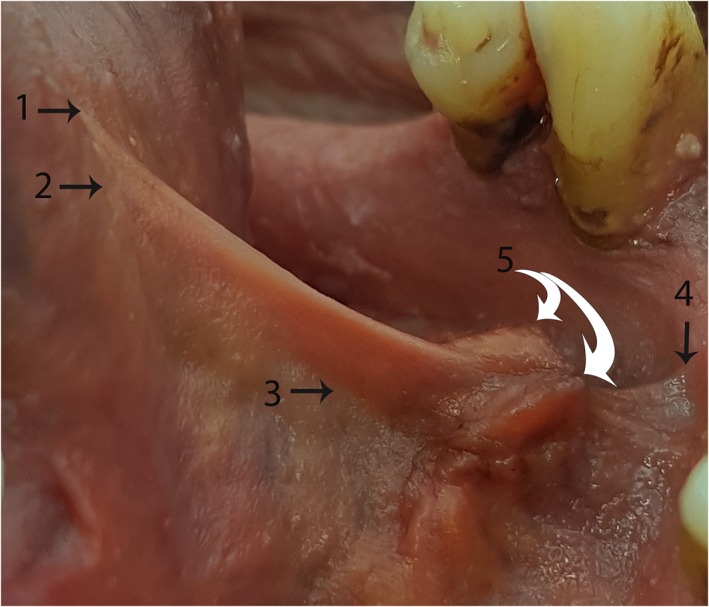
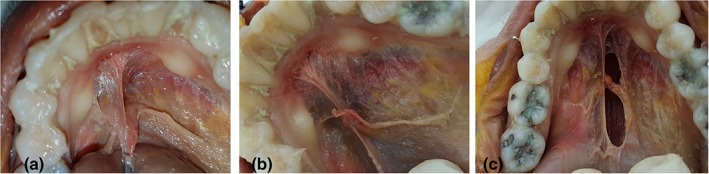
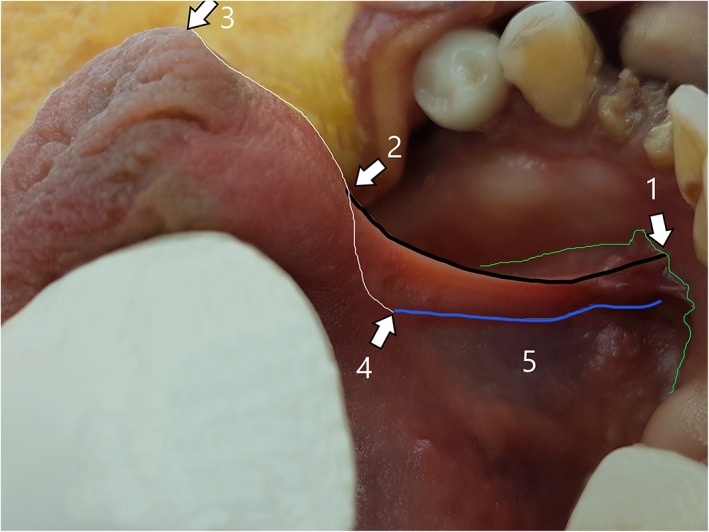
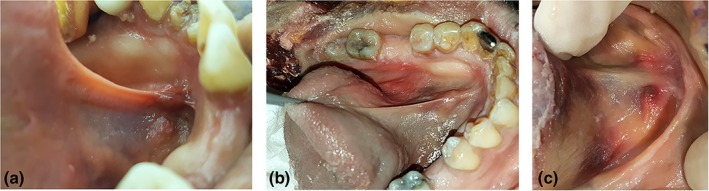
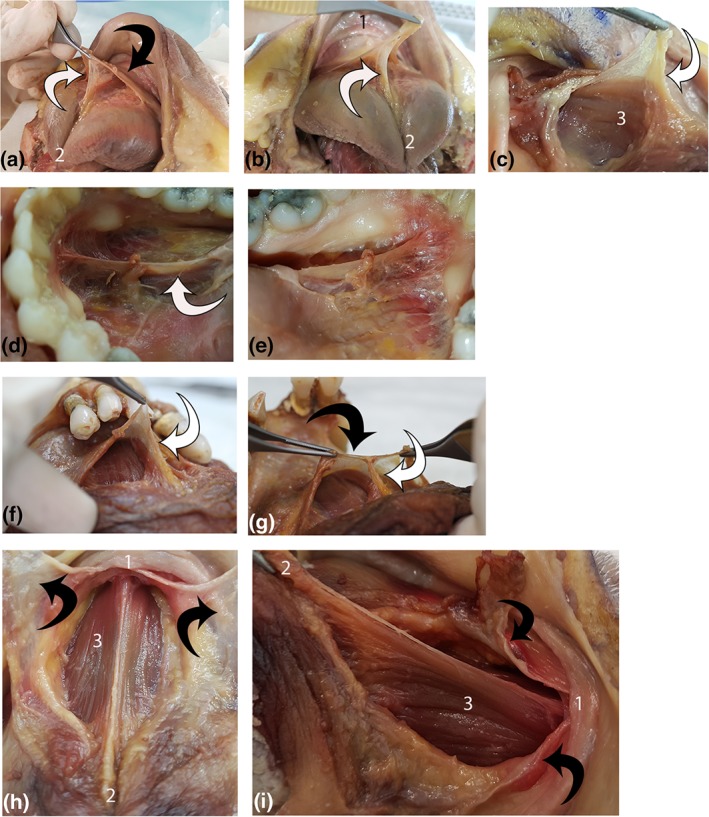
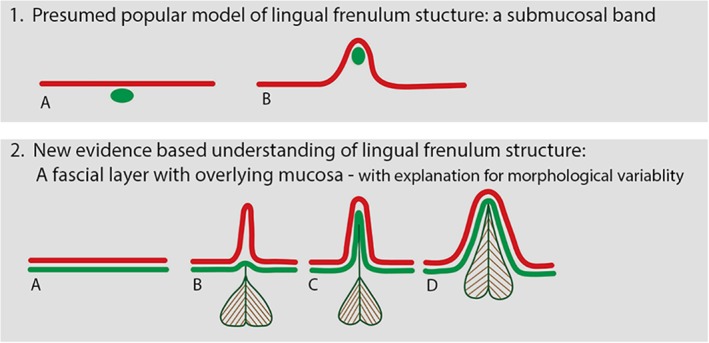
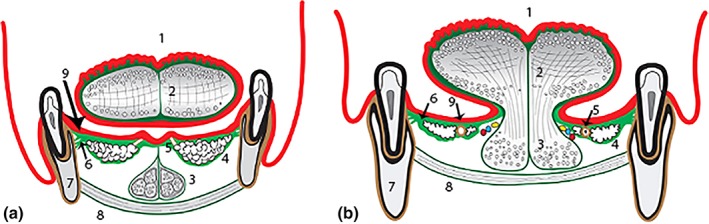
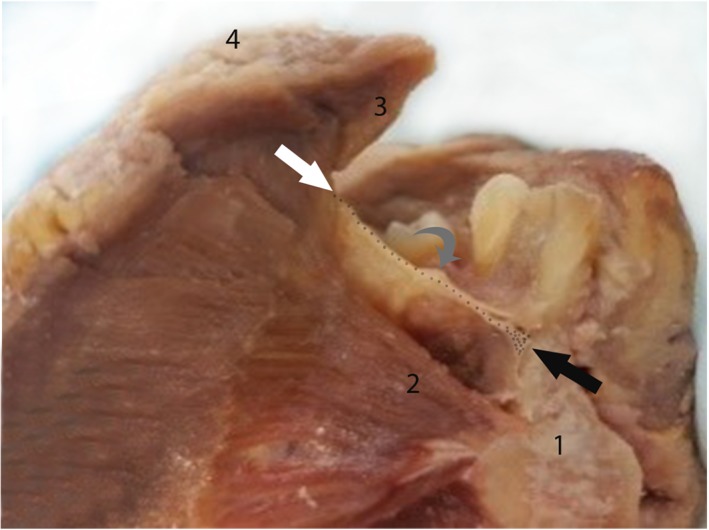
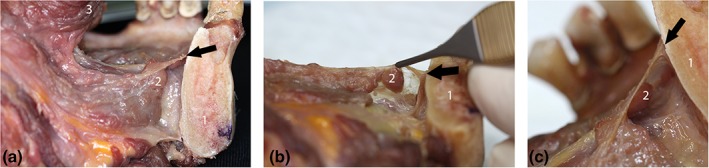
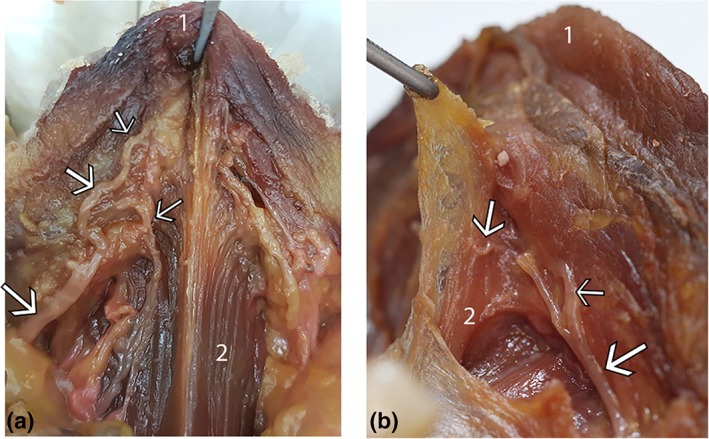
Surgical release of the lingual frenulum (frenotomy) has become an increasingly common procedure, performed from birth through to adulthood. Surprisingly, detailed anatomy of the in-situ lingual frenulum has never been described, and no anatomical basis has been proposed for the individual variability in frenulum morphology. The lingual frenulum is frequently referred to as a "cord" or "submucosal band" of connective tissue, yet there is no evidence to support this anatomical construct. This paper aims to describe the anatomy of the in-situ lingual frenulum and its relationship to floor of mouth structures. Fresh tissue microdissection of the lingual frenulum and floor of mouth was performed on nine adult cadavers with photo-documentation and description of findings. The lingual frenulum is a dynamic structure, formed by a midline fold in a layer of fascia that inserts around the inner arc of the mandible, forming a diaphragm-like structure across the floor of mouth. This fascia is located immediately beneath the oral mucosa, fusing centrally with the connective tissue on the tongue's ventral surface. The sublingual glands and submandibular ducts are enveloped by the fascial layer and anterior genioglossus fibers are suspended beneath it. Lingual nerve branches are located superficially on the ventral surface of the tongue, immediately deep to the fascia. The lingual frenulum is not a discrete midline structure. It is formed by dynamic elevation of a midline fold in the floor of mouth fascia. With this study, the clinical concept of ankyloglossia and its surgical management warrant revision. Clin. Anat. 32:749-761, 2019. © 2019 The Authors. Clinical Anatomy published by Wiley Periodicals, Inc. on behalf of American Association of Clinical Anatomists.
Keywords: ankyloglossia; congenital; fascia; floor of mouth; frenotomy; lingual frenulum; lingual nerve; oral cavity; tongue tie.
© 2019 The Authors. Clinical Anatomy published by Wiley Periodicals, Inc. on behalf of American Association of Clinical Anatomists.
Figures


References
-
- Baker A. 2015. Surgical treatment of ankyloglossia. Oper Tech Otolaryngol Head Neck Surg 26:28–32.
-
- Chu MW, Bloom DC. 2009. Posterior ankyloglossia: A case report. Int J Pediatr Otorhinolaryngol 73:881–883. - PubMed
-
- Coryllos E, Watson Genna, C , Salloum A. 2004. Congenital tongue tie and its impact on breastfeeding. American Academy of Pediatrics (Summer): Breastfeeding: Best for Mother and Baby:1–6.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
