

Growing evidence of Plasmodium vivax across malaria-endemic Africa
- PMID: 30703083
- PMCID: PMC6372205
- DOI: 10.1371/journal.pntd.0007140
Growing evidence of Plasmodium vivax across malaria-endemic Africa
Erratum in
-
Correction: Growing evidence of Plasmodium vivax across malaria-endemic Africa.PLoS Negl Trop Dis. 2019 Jun 28;13(6):e0007525. doi: 10.1371/journal.pntd.0007525. eCollection 2019 Jun. PLoS Negl Trop Dis. 2019. PMID: 31251740 Free PMC article.
Abstract
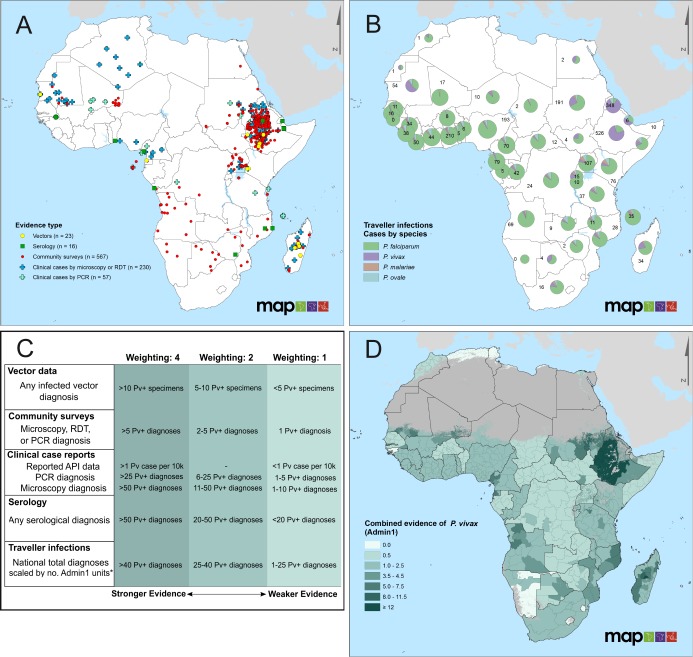
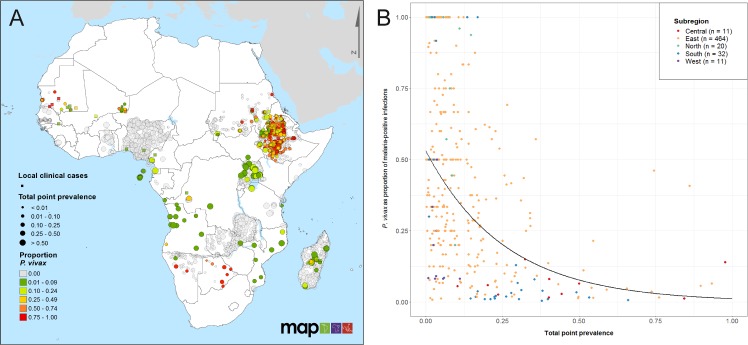
Effective malaria control strategies require an accurate understanding of the epidemiology of locally transmitted Plasmodium species. Compared to Plasmodium falciparum infection, Plasmodium vivax has a lower asexual parasitaemia, forms dormant liver-stages (hypnozoites), and is more transmissible. Hence, treatment and diagnostic policies aimed exclusively at P. falciparum are far less efficient against endemic P. vivax. Within sub-Saharan Africa, malaria control programmes justly focus on reducing the morbidity and mortality associated with P. falciparum. However, the recent emphasis on malaria elimination and increased accessibility of more sensitive diagnostic tools have revealed greater intricacies in malaria epidemiology across the continent. Since 2010, the number of studies identifying P. vivax endemic to Africa has expanded considerably, with 88 new scientific reports published since a review of evidence in 2015, approximately doubling the available data. There is evidence of P. vivax in all regions of Africa, apparent from infected vectors, clinical cases, serological indicators, parasite prevalence, exported infections, and P. vivax-infected Duffy-negative individuals. Where the prevalence of microscopic parasitaemia is low, a greater proportion of P. vivax infections were observed relative to P. falciparum. This evidence highlights an underlying widespread presence of P. vivax across all malaria-endemic regions of Africa, further complicating the current practical understanding of malaria epidemiology in this region. Thus, ultimate elimination of malaria in Africa will require national malaria control programmes to adopt policy and practice aimed at all human species of malaria.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Bhatt S, Weiss DJ, Cameron E, Bisanzio D, Mappin B, Dalrymple U, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature. 2015;526:207 10.1038/nature15535 https://www.nature.com/articles/nature15535#supplementary-information. - DOI - PMC - PubMed
-
- WHO. World Malaria Report 2017 Geneva, Switzerland: World Health Organization, 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
