

Predictors of long-term prognosis in acute kidney injury survivors who require continuous renal replacement therapy after cardiovascular surgery
- PMID: 30703146
- PMCID: PMC6355115
- DOI: 10.1371/journal.pone.0211429
Predictors of long-term prognosis in acute kidney injury survivors who require continuous renal replacement therapy after cardiovascular surgery
Abstract
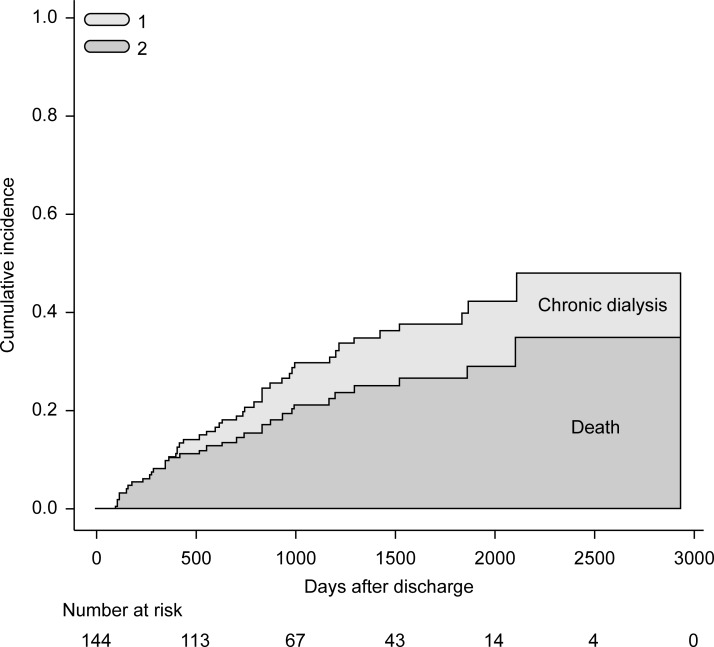
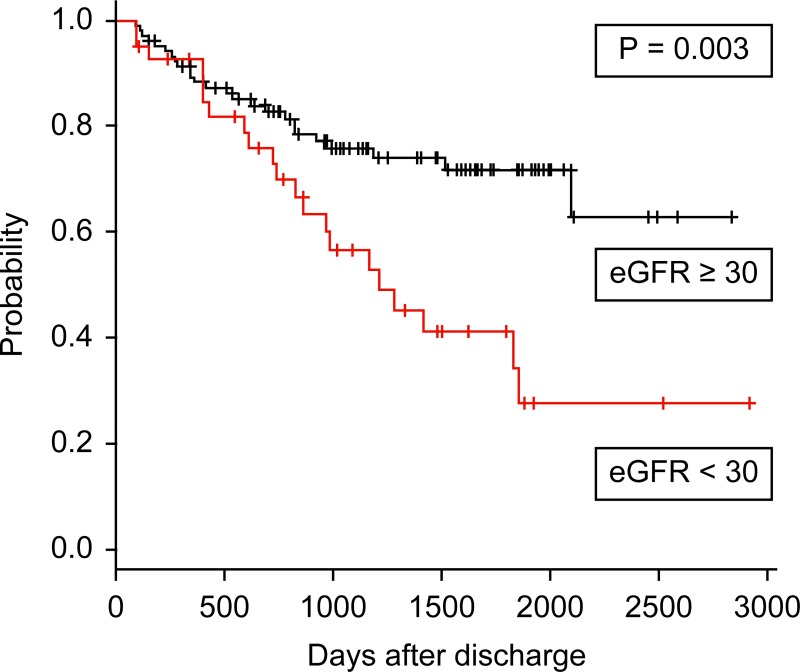
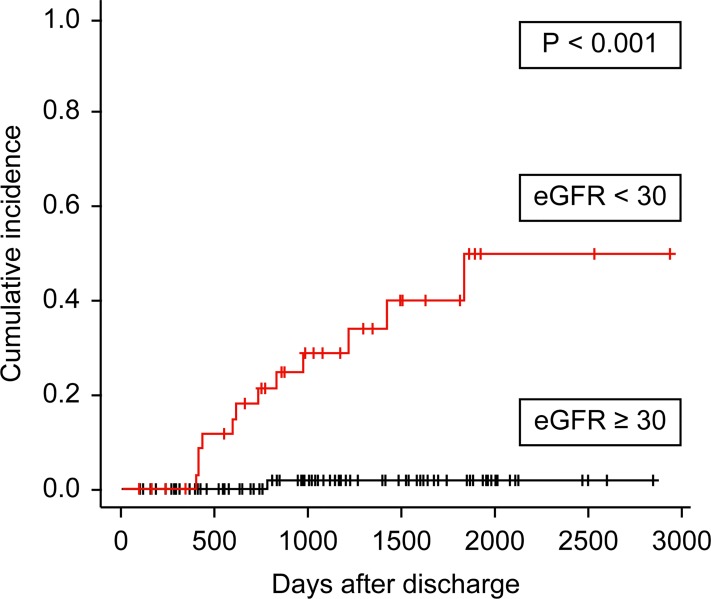
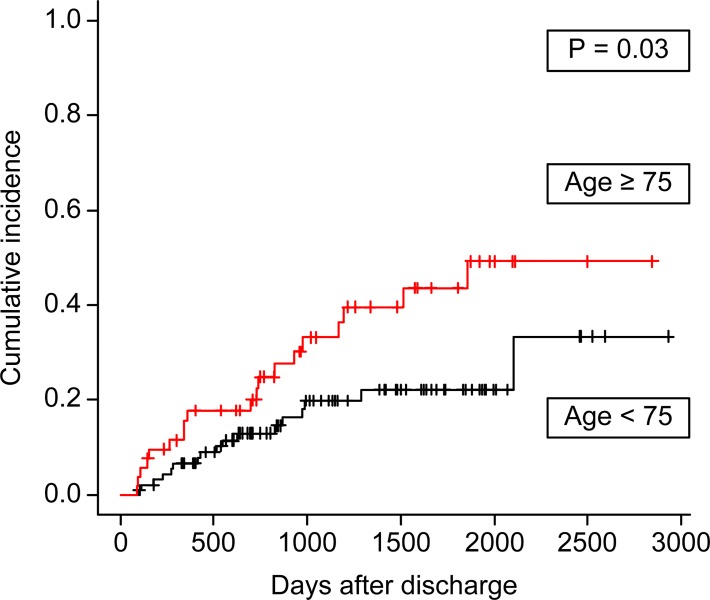
The long-term prognosis of patients with postoperative acute kidney injury (AKI) requiring continuous renal replacement therapy (CRRT) after cardiovascular surgery is unclear. We aimed to investigate long-term renal outcomes and survival in these patients to determine the risk factors for negative outcomes. Long-term prognosis was examined in 144 hospital survivors. All patients were independent and on renal replacement therapy at hospital discharge. The median age at operation was 72.0 years, and the median pre-operative estimated glomerular filtration rate (eGFR) was 39.5 mL/min/1.73 m2. The median follow-up duration was 1075 days. The endpoints were death, chronic maintenance dialysis dependence, and a composite of death and chronic dialysis. Predictors for death and dialysis were evaluated using Fine and Gray's competing risk analysis. The cumulative incidence of death was 34.9%, and the chronic dialysis rate was 13.3% during the observation period. In the multivariate proportional hazards analysis, eGFR <30 mL/min/1.73 m2 at discharge was associated with the composite endpoint of death and dialysis [hazard ratio (HR), 2.1; 95% confidence interval (CI), 1.1-3.8; P = 0.02]. Hypertension (HR 8.7, 95% CI, 2.2-35.4; P = 0.002) and eGFR <30 mL/min/1.73 m2 at discharge (HR 26.4, 95% CI, 2.6-267.1; P = 0.006) were associated with dialysis. Advanced age (≥75 years) was predictive of death. Patients with severe CRRT-requiring AKI after cardiovascular surgery have increased risks of chronic dialysis and death. Patients with eGFR <30 mL/min/1.73 m2 at discharge should be monitored especially carefully by nephrologists due to the risk of chronic dialysis and death.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The impact of continuous renal replacement therapy on renal outcomes in dialysis-requiring acute kidney injury may be related to the baseline kidney function.BMC Nephrol. 2017 May 3;18(1):150. doi: 10.1186/s12882-017-0564-z. BMC Nephrol. 2017. PMID: 28464841 Free PMC article.
-
Impaired kidney function at hospital discharge and long-term renal and overall survival in patients who received CRRT.Clin J Am Soc Nephrol. 2013 Aug;8(8):1284-91. doi: 10.2215/CJN.06650712. Epub 2013 Apr 18. Clin J Am Soc Nephrol. 2013. PMID: 23599403 Free PMC article.
-
Kidney function decline after a non-dialysis-requiring acute kidney injury is associated with higher long-term mortality in critically ill survivors.Crit Care. 2012 Jul 12;16(4):R123. doi: 10.1186/cc11419. Crit Care. 2012. PMID: 22789111 Free PMC article.
-
Recovery after Critical Illness and Acute Kidney Injury.Clin J Am Soc Nephrol. 2021 Oct;16(10):1601-1609. doi: 10.2215/CJN.19601220. Epub 2021 Aug 30. Clin J Am Soc Nephrol. 2021. PMID: 34462285 Free PMC article. Review.
-
Permissive hypofiltration.Crit Care. 2012 Jul 26;16(4):317. doi: 10.1186/cc11253. Crit Care. 2012. PMID: 22839207 Free PMC article. Review.
Cited by
-
Impact of protocolized diuresis for de-resuscitation in the intensive care unit.Crit Care. 2020 Feb 28;24(1):70. doi: 10.1186/s13054-020-2795-9. Crit Care. 2020. PMID: 32111247 Free PMC article.
-
Postoperative anemia is a risk factor for acute kidney injury after open aorta and vena cava surgeries.PLoS One. 2020 Oct 13;15(10):e0240243. doi: 10.1371/journal.pone.0240243. eCollection 2020. PLoS One. 2020. PMID: 33048948 Free PMC article.
-
Risk factors for adverse short-term and long-term outcomes in children with severe acute kidney injury requiring continuous kidney replacement therapy.Pediatr Nephrol. 2025 Aug;40(8):2679-2690. doi: 10.1007/s00467-025-06753-x. Epub 2025 Apr 11. Pediatr Nephrol. 2025. PMID: 40214781
-
Continuous renal replacement therapy in elderly with acute kidney injury.Korean J Intern Med. 2020 Mar;35(2):284-294. doi: 10.3904/kjim.2019.431. Epub 2020 Feb 28. Korean J Intern Med. 2020. PMID: 32131572 Free PMC article. Review.
-
Urinary Spermidine Predicts and Associates with In-Hospital Acute Kidney Injury after Cardiac Surgery.Antioxidants (Basel). 2021 Jun 2;10(6):896. doi: 10.3390/antiox10060896. Antioxidants (Basel). 2021. PMID: 34199603 Free PMC article.
References
-
- Newsome BB, Warnock DG, McClellan WM, Herzog CA, Kiefe CI, Eggers PW, et al. Long-term risk of mortality and end-stage renal disease among the elderly after small increases in serum creatinine level during hospitalization for acute myocardial infarction. Arch Intern Med. 2008;168: 609–616. 10.1001/archinte.168.6.609 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
