

Utility of Indocyanine Green Angiography to Identify Clinical Factors Associated With Perfusion of Paramedian Forehead Flaps During Nasal Reconstruction Surgery
- PMID: 30703191
- PMCID: PMC6537837
- DOI: 10.1001/jamafacial.2018.1829
Utility of Indocyanine Green Angiography to Identify Clinical Factors Associated With Perfusion of Paramedian Forehead Flaps During Nasal Reconstruction Surgery
Abstract
Importance: Identifying factors affecting forehead flap neovascularization during nasal reconstruction surgical procedures using quantitative dynamics of fluorescence from indocyanine green angiography may be associated with reduced vascular complications.
Objectives: To identify quantifiable forehead flap perfusion measures using indocyanine green angiography during nasal reconstruction procedures and to evaluate clinical factors associated with neovascularization.
Design, setting, and participants: Retrospective cohort study of 71 patients at a tertiary referral center of Stanford University, Stanford, California, between January 1, 2010, and March 31, 2018, undergoing forehead flap nasal reconstruction surgery with flap perfusion assessed by indocyanine green angiography.
Exposures: Indocyanine green angiography was performed intraoperatively to record forehead flap neovascularization during the second stage of nasal reconstruction surgery after temporary clamping of the pedicle.
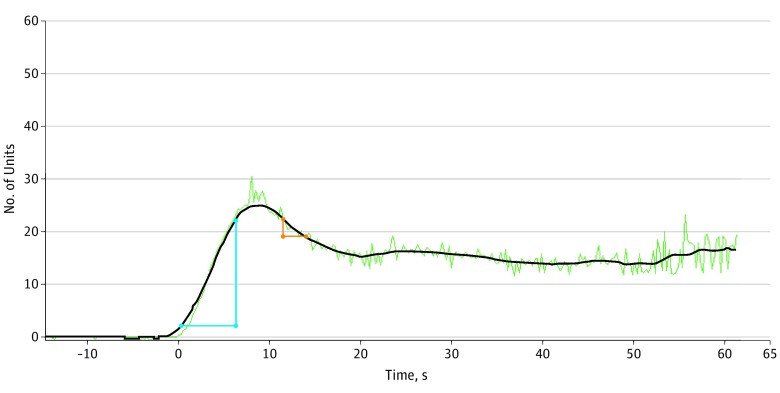
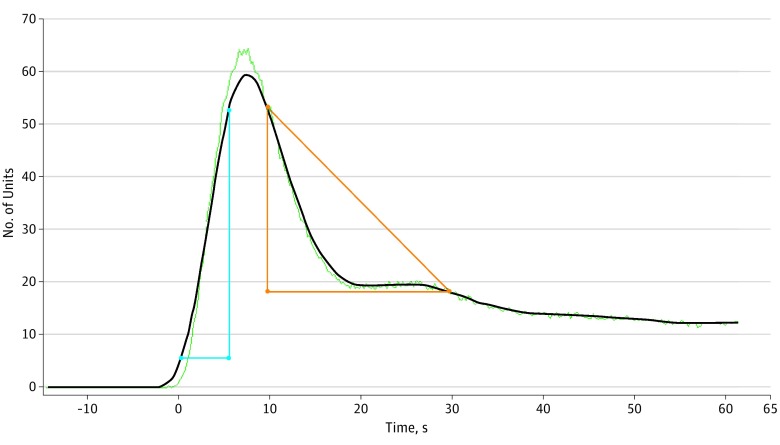
Main outcomes and measures: With use of quantifiable data of fluorescence dynamics, flap perfusion in association with a reference point in the cheek after pedicle clamping was assessed by 2 methods: (1) ingress (arterial inflow) and egress (venous outflow) flap-to-cheek ratio and (2) flap-to-cheek perfusion (fluorescence) ratio at 3 time points (midpoint of indocyanine green flap inflow, maximum fluorescence [peak], and midpoint of indocyanine green flap outflow) and their calculated mean. Association of the perfusion measures with patient and procedural factors was performed using linear regression models.
Results: Of the 71 patients included in the study, 43 (61%) were men; the mean (SD) age was 71.1 (11.0) years. The mean (SD) flap-to-cheek inflow ratio was 0.48 (0.40), peak fluorescence ratio was 0.59 (0.34), and outflow ratio was 0.88 (0.42). The calculated mean (SD) flap-to-cheek perfusion ratio of these measures was 0.65 (0.35). The mean (SD) flap-to-cheek ingress ratio was 0.54 (0.36) and egress ratio was 0.65 (0.98). With use of a multivariable regression model, the time between stages was positively associated with flap-to-cheek ingress ratio (β, 0.015; 95% CI, 0.001 to 0.030), and cartilage grafting was negatively associated with flap-to-cheek outflow ratio (β, -0.240; 95% CI, -0.472 to -0.008).
Conclusions and relevance: The findings suggest that indocyanine green angiography is an effective method to quantify relative neovascularization perfusion of forehead flaps. Future applications may include the use of this technology to aid in early flap division and ensure adequate perfusion among high-risk patients.
Level of evidence: NA.
Conflict of interest statement
Figures
References
-
- Burget GC. Aesthetic restoration of the nose. Clin Plast Surg. 1985;12(3):463-480. - PubMed
-
- Hessam S, Georgas D, Sand M, Bechara FG. Penetrating defect of the ala nasi: combined reconstruction with a myocutaneous hinge- and paramedian forehead flap. J Dtsch Dermatol Ges. 2014;12(2):169-171. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials