

Derivation of Anthracycline and Anthraquinone Equivalence Ratios to Doxorubicin for Late-Onset Cardiotoxicity
- PMID: 30703192
- PMCID: PMC6490232
- DOI: 10.1001/jamaoncol.2018.6634
Derivation of Anthracycline and Anthraquinone Equivalence Ratios to Doxorubicin for Late-Onset Cardiotoxicity
Abstract
Importance: Anthracyclines are part of many effective pediatric cancer treatment protocols. Most pediatric oncology treatment groups assume that the hematologic toxicity of anthracycline agents is equivalent to their cardiotoxicity; for example, Children's Oncology Group substitution rules consider daunorubicin and epirubicin isoequivalent to doxorubicin, whereas mitoxantrone and idarubicin are considered 4 to 5 times as toxic as doxorubicin.
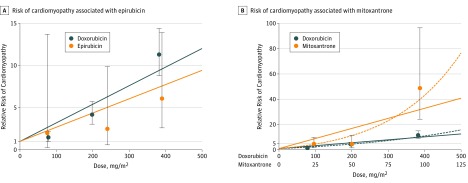
Objective: To determine optimal dose equivalence ratios for late-onset cardiomyopathy between doxorubicin and other anthracyclines or the anthraquinone mitoxantrone.
Design, setting, and participants: This multicenter cohort study of childhood cancer survivors who survived 5 or more years analyzed data pooled from 20 367 participants in the Childhood Cancer Survivor Study treated from 1970 to 1999, 5741 participants in the Dutch Childhood Oncology Group LATER study diagnosed between 1963 and 2001, and 2315 participants in the St Jude Lifetime study treated from 1962 to 2005.
Exposures: Cumulative doses of each agent (the anthracyclines doxorubicin, daunorubicin, epirubicin, and idarubicin; and the anthraquinone mitoxantrone) along with chest radiotherapy exposure were abstracted from medical records.
Main outcomes and measures: Cardiomyopathy (severe, life-threatening, or fatal) by 40 years of age. Agent-specific Cox proportional hazards models evaluated cardiomyopathy risk, adjusting for chest radiotherapy, age at cancer diagnosis, sex, and exposure to anthracyclines or to an anthraquinone. An agent-specific cardiomyopathy equivalence ratio (relative to doxorubicin) was estimated for each dose category as a ratio of the hazard ratios, and then a weighted mean determined the overall agent-specific equivalence ratio across all dose categories.
Results: Of 28 423 survivors (46.4% female; median age at cancer diagnosis 6.1 years [range, 0.0-22.7 years]), 9330 patients received doxorubicin, 4433 received daunorubicin, 342 received epirubicin, 241 received idarubicin, and 265 received mitoxantrone. After a median follow-up of 20.0 years (range, 5.0-40.0 years) following receipt of a cancer diagnosis, 399 cardiomyopathy cases were observed. Relative to doxorubicin, the equivalence ratios were 0.6 (95% CI, 0.4-1.0) for daunorubicin, 0.8 (95% CI, 0.5-2.8) for epirubicin, and 10.5 (95% CI, 6.2-19.1) for mitoxantrone. Outcomes were too rare to generate idarubicin-specific estimates. Ratios based on a continuous linear dose-response relationship were similar for daunorubicin (0.5 [95% CI, 0.4-0.7]) and epirubicin (0.8 [95% CI, 0.3-1.4]). The relationship between mitoxantrone and doxorubicin appeared better characterized by a linear exponential model.
Conclusions and relevance: In a large data set assembled to examine long-term cardiomyopathy risk in childhood cancer survivors, daunorubicin was associated with decreased cardiomyopathy risk vs doxorubicin, whereas epirubicin was approximately isoequivalent. By contrast, the current hematologic-based doxorubicin dose equivalency of mitoxantrone (4:1) appeared to significantly underestimate the association of mitoxantrone with long-term cardiomyopathy risk.
Figures
References
-
- Lipshultz SE, Adams MJ, Colan SD, et al. . Long-term cardiovascular toxicity in children, adolescents, and young adults who receive cancer therapy: pathophysiology, course, monitoring, management, prevention, and research directions: a scientific statement from the American Heart Association. Circulation. 2013;128(17):1927-1995. doi:10.1161/CIR.0b013e3182a88099 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
