

Differences in Receipt of Alcohol-Related Care Across Rurality Among VA Patients Living With HIV With Unhealthy Alcohol Use
- PMID: 30703856
- PMCID: PMC6639081
- DOI: 10.1111/jrh.12345
Differences in Receipt of Alcohol-Related Care Across Rurality Among VA Patients Living With HIV With Unhealthy Alcohol Use
Abstract
Purpose: It is unknown whether receipt of evidence-based alcohol-related care varies by rurality among people living with HIV (PLWH) with unhealthy alcohol use-a population for whom such care is particularly important.
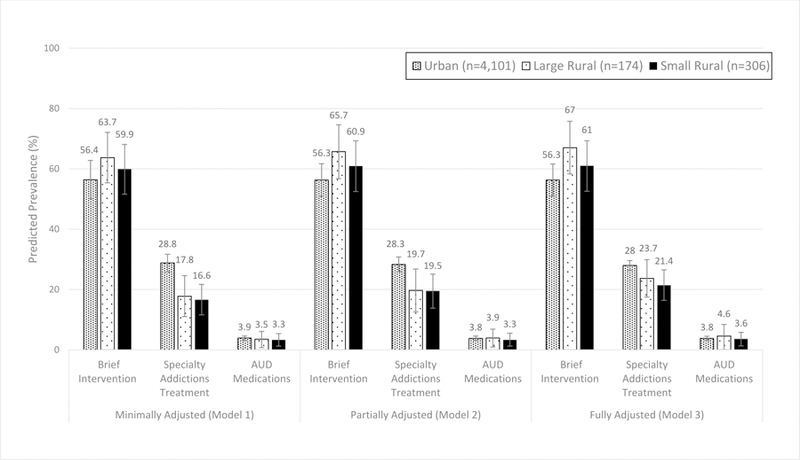
Methods: All positive screens for unhealthy alcohol use (AUDIT-C ≥ 5) among PLWH were identified using Veterans Health Administration electronic health record data (10/1/09-5/30/13). Three domains of alcohol-related care were assessed: brief intervention (BI) within 14 days, and specialty addictions treatment or alcohol use disorder (AUD) medications (filled prescription for naltrexone, disulfiram, acamprosate, or topiramate) within 1 year of positive screen. Adjusted Poisson models and recycled predictions were used to estimate predicted prevalence of outcomes across rurality (urban, large rural, small rural), clustered on facility. Secondary analyses assessed outcomes in the subsample with documented AUD.
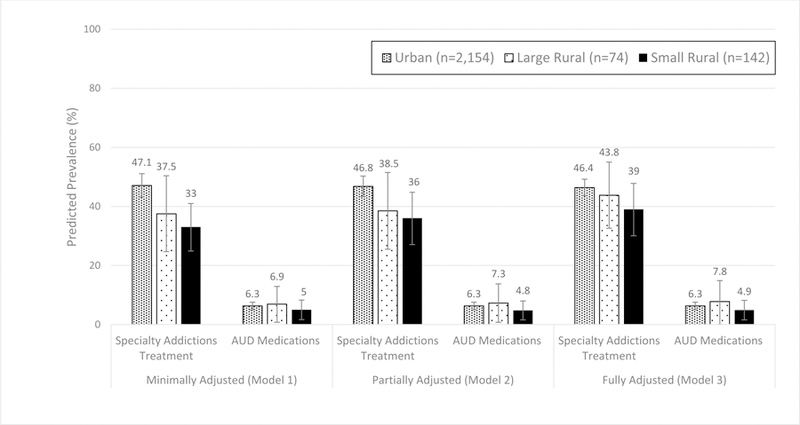
Findings: 4,581 positive screens representing 3,458 PLWH (3,112 urban, 130 large rural, and 216 small rural) were included; 49.1% had diagnosed AUD. PLWH in large rural areas had highest receipt of BI (urban 56.6%, 95% CI: 55.0-58.2; large rural 66.0%, CI: 58.6-73.5; small rural 60.7%, CI: 54.6-67.0). PLWH in urban areas had highest receipt of specialty addictions treatment (urban 28.2%, CI: 26.7-29.8; large rural 19.7%, CI: 13.1-26.2; small rural 19.6%, CI: 14.1-25.0). There was no difference in receipt of AUD medications, although overall receipt was low (3%-4%). Results were similar in the subsample with AUD.
Conclusion: Among PLWH with unhealthy alcohol use, those in rural areas may be vulnerable to under-receipt of specialty addictions treatment. Targeted interventions may help ensure PLWH receive recommended care regardless of rurality.
Keywords: HIV; alcohol-related care; rural; urban; veterans.
© 2019 National Rural Health Association.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
