

Clinical Events After Deferral of LAD Revascularization Following Physiological Coronary Assessment
- PMID: 30704577
- PMCID: PMC6354033
- DOI: 10.1016/j.jacc.2018.10.070
Clinical Events After Deferral of LAD Revascularization Following Physiological Coronary Assessment
Abstract
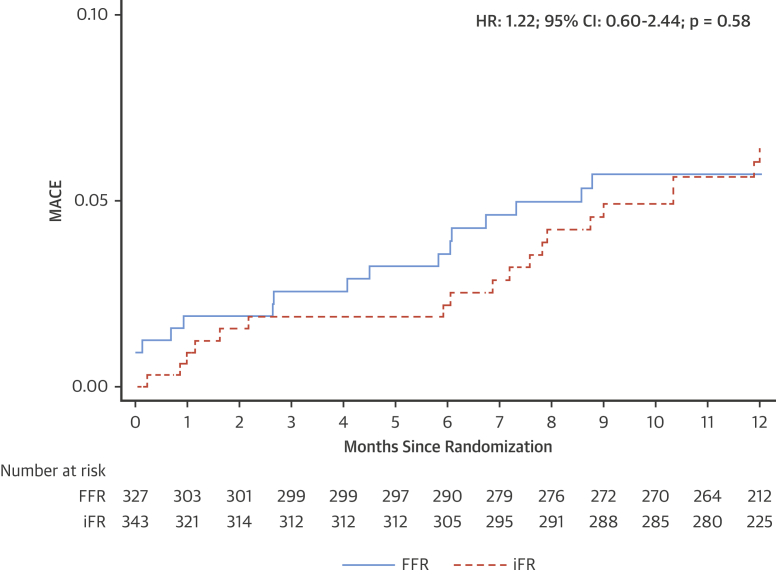
Background: Physicians are not always comfortable deferring treatment of a stenosis in the left anterior descending (LAD) artery because of the perception that there is a high risk of major adverse cardiac events (MACE). The authors describe, using the DEFINE-FLAIR (Functional Lesion Assessment of Intermediate Stenosis to Guide Revascularisation) trial, MACE rates when LAD lesions are deferred, guided by physiological assessment using fractional flow reserve (FFR) or the instantaneous wave-free ratio (iFR).
Objectives: The purpose of this study was to establish the safety of deferring treatment in the LAD using FFR or iFR within the DEFINE-FLAIR trial.
Methods: MACE rates at 1 year were compared between groups (iFR and FFR) in patients whose physiological assessment led to LAD lesions being deferred. MACE was defined as a composite of cardiovascular death, myocardial infarction (MI), and unplanned revascularization at 1 year. Patients, and staff performing follow-up, were blinded to whether the decision was made with FFR or iFR. Outcomes were adjusted for age and sex.
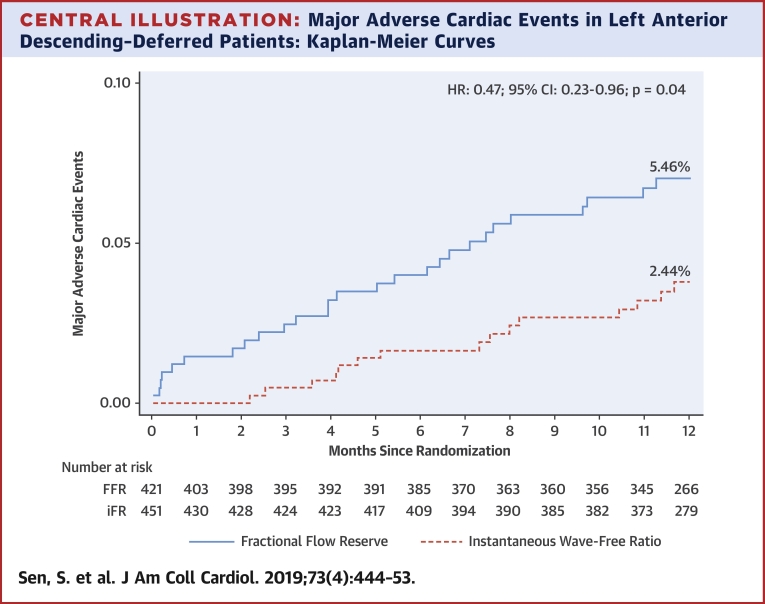
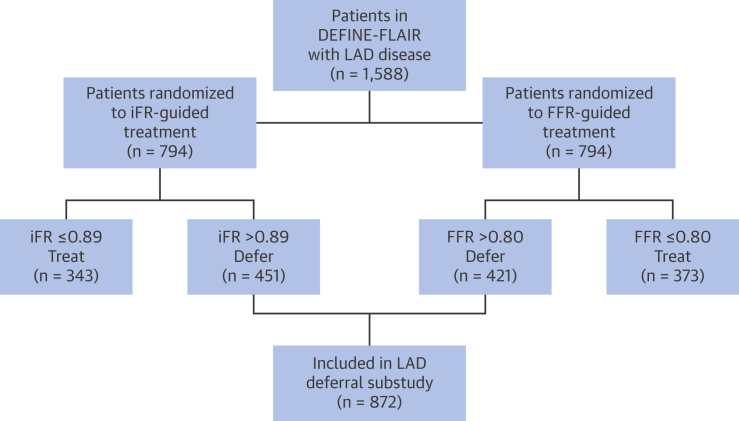
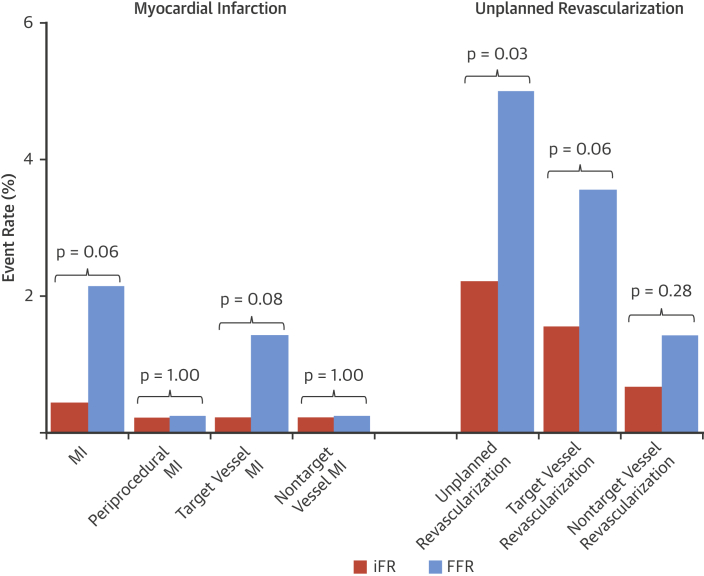
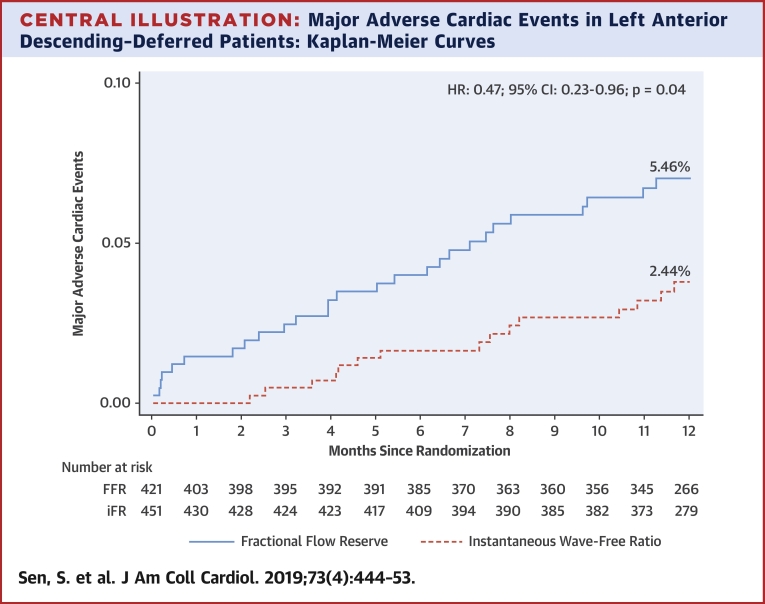
Results: A total of 872 patients had lesions deferred in the LAD (421 guided by FFR, 451 guided by iFR). The event rate with iFR was significantly lower than with FFR (2.44% vs. 5.26%; adjusted HR: 0.46; 95% confidence interval [CI]: 0.22 to 0.95; p = 0.04). This was driven by significantly lower unplanned revascularization with iFR and numerically lower MI (unplanned revascularization: 2.22% iFR vs. 4.99% FFR; adjusted HR: 0.44; 95% CI: 0.21 to 0.93; p = 0.03; MI: 0.44% iFR vs. 2.14% FFR; adjusted HR: 0.23; 95% CI: 0.05 to 1.07; p = 0.06).
Conclusions: iFR-guided deferral appears to be safe for patients with LAD lesions. Patients in whom iFR-guided deferral was performed had statistically significantly lower event rates than those with FFR-guided deferral.
Keywords: coronary stenosis; fractional flow reserve; instantaneous wave-free ratio.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Family of Flow Reserve Indexes and Coronary Revascularization: Miles to Go Before We Sleep.J Am Coll Cardiol. 2019 Feb 5;73(4):454-456. doi: 10.1016/j.jacc.2018.12.005. J Am Coll Cardiol. 2019. PMID: 30704578 No abstract available.
References
-
- Sen S., Escaned J., Malik I.S. Development and validation of a new adenosine-independent index of stenosis severity from coronary wave-intensity analysis: results of the ADVISE (ADenosine Vasodilator Independent Stenosis Evaluation) study. J Am Coll Cardiol. 2012;59:1392–1402. - PubMed
-
- Davies J.E., Sen S., Dehbi H.-M. Use of the instantaneous wave-free ratio or fractional flow reserve in PCI. N Engl J Med. 2017;376:1824–1834. - PubMed
-
- Götberg M., Christiansen E.H., Gudmundsdottir I.J. Instantaneous wave-free ratio versus fractional flow reserve to guide PCI. N Engl J Med. 2017;376:1813–1823. - PubMed
-
- Greenbaum A.B., Califf R.M., Jones R.H. Comparison of medicine alone, coronary angioplasty, and left internal mammary artery-coronary artery bypass for one-vessel proximal left anterior descending coronary artery disease. Am J Cardiol. 2000;86:1322–1326. - PubMed
-
- Kobayashi Y., Johnson N.P., Berry C. The influence of lesion location on the diagnostic accuracy of adenosine-free coronary pressure wire measurements. J Am Coll Cardiol Intv. 2016;9:2390–2399. - PubMed
