

Mortality and Kidney Transplantation Outcomes Among Hepatitis C Virus-Seropositive Maintenance Dialysis Patients: A Retrospective Cohort Study
- PMID: 30704882
- PMCID: PMC6535135
- DOI: 10.1053/j.ajkd.2018.11.009
Mortality and Kidney Transplantation Outcomes Among Hepatitis C Virus-Seropositive Maintenance Dialysis Patients: A Retrospective Cohort Study
Abstract
Rationale & objective: Hepatitis C virus (HCV) infection is common among maintenance dialysis patients. Few studies have examined both dialysis survival and transplantation outcomes for HCV-seropositive patients because registry data sets lack information for HCV serostatus.
Study design: Retrospective cohort study.
Setting & participants: Adult long-term dialysis patients treated by a US national dialysis provider between January 1, 2004, and December 31, 2014.
Exposure: HCV antibody serostatus obtained as part of clinical data from a national dialysis provider.
Outcomes: Mortality on dialysis therapy, entry onto the kidney transplant waiting list, kidney transplantation, and estimated survival benefit from kidney transplantation versus remaining on the waitlist.
Analytical approach: After linking clinical data with data from the Organ Procurement and Transplantation Network, Cox and cause-specific hazards regression were implemented to estimate the associations between HCV seropositivity and mortality, as well as entry onto the kidney transplant waitlist. Cox regression was also used to estimate the survival benefit from transplantation versus dialysis among HCV-seropositive individuals.
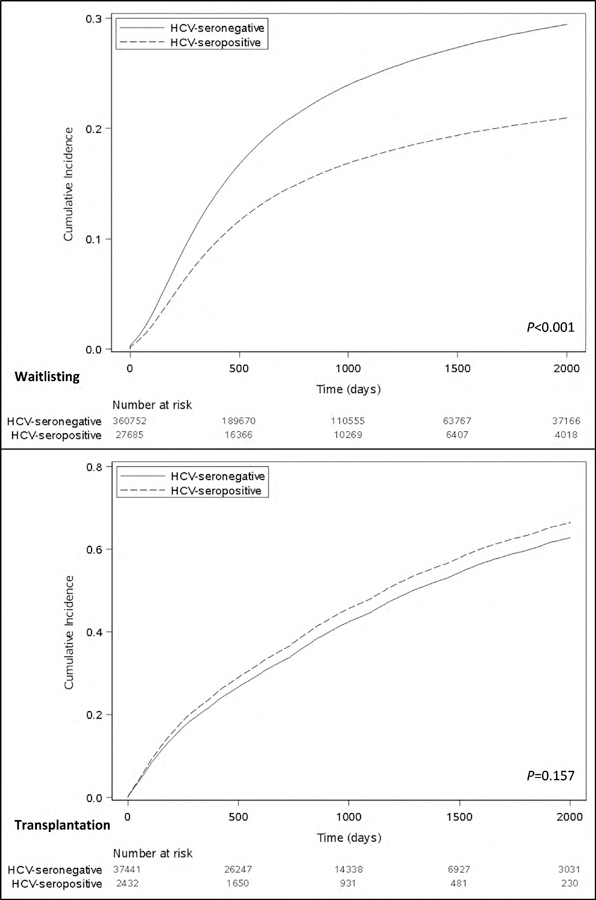
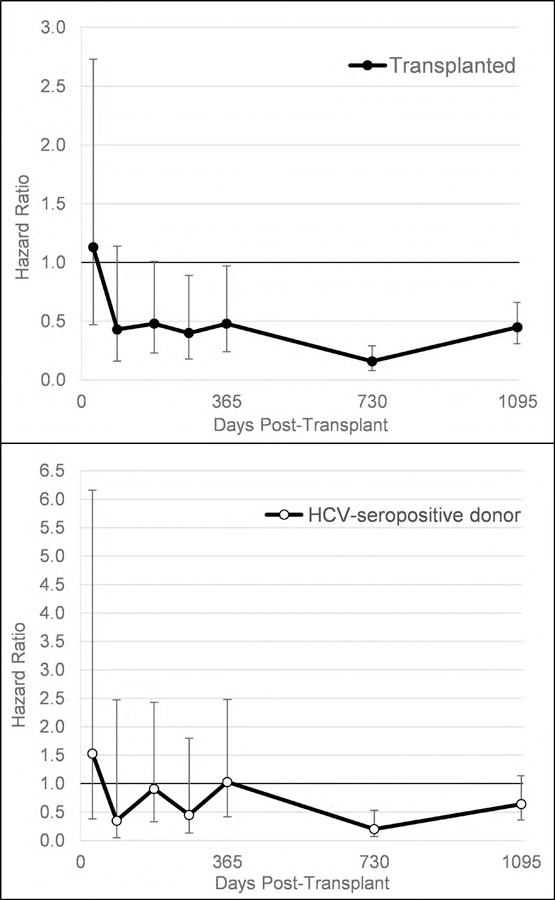
Results: Among 442,171 dialysis patients, 31,624 (7.2%) were HCV seropositive. HCV seropositivity was associated with a small elevation in the rate of death (adjusted HR [aHR], 1.09; 95% CI, 1.07-1.11) and a substantially lower rate of entry onto the kidney transplant waitlist (subdistribution HR [sHR], 0.67; 95% CI, 0.61-0.74). Once wait-listed, the kidney transplantation rate was not different for HCV-seropositive (sHR 1.10; 95% CI, 0.96-1.27) versus HCV-seronegative patients. HCV-seropositive patients lived longer with transplantation (aHR at 3 years, 0.42; 95% CI, 0.27-0.63). Receiving an HCV-seropositive donor kidney provided a survival advantage at the 2-year posttransplantation time point compared to remaining on dialysis therapy waiting for an HCV-negative kidney.
Limitations: No data for HCV viral load or liver biopsy.
Conclusions: HCV-seropositive patients experience reduced access to the kidney transplantation waitlist despite deriving a substantial survival benefit from transplantation. HCV-seropositive patients should consider foregoing HCV treatment while accepting kidneys from HCV-infected donors to facilitate transplantation and prolong survival.
Trial registration: ClinicalTrials.gov NCT02743897.
Keywords: Dialysis; ESRD modality; HCV seropositive; barriers to transplantation; chronic kidney disease (CKD); delisting; end-stage renal disease (ESRD); hepatitis C virus (HCV); kidney transplantation; survival benefit; waitlisting.
Copyright © 2019 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Fabrizi F, Bunnapradist S, Lunghi G, Aucella F, Martin P. Epidemiology and clinical significance of hepatotropic infections in dialysis patients. Recent evidence. Minerva urologica e nefrologica = The Italian journal of urology and nephrology 2004;56(3):249–257. - PubMed
-
- Schneeberger PM, Keur I, van Loon AM, et al. The prevalence and incidence of hepatitis C virus infections among dialysis patients in the Netherlands: a nationwide prospective study. The Journal of infectious diseases 2000;182(5):1291–1299. - PubMed
-
- Saab S, Martin P, Brezina M, Gitnick G, Yee HF Jr., Serum alanine aminotransferase in hepatitis c screening of patients on hemodialysis. American journal of kidney diseases : the official journal of the National Kidney Foundation 2001;37(2):308–315. - PubMed
-
- Kalantar-Zadeh K, Kilpatrick RD, McAllister CJ, et al. Hepatitis C virus and death risk in hemodialysis patients. J Am Soc Nephrol 2007;18(5):1584–1593. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
