

IgG4-related disease: what a hematologist needs to know
- PMID: 30705099
- PMCID: PMC6395313
- DOI: 10.3324/haematol.2018.205526
IgG4-related disease: what a hematologist needs to know
Abstract
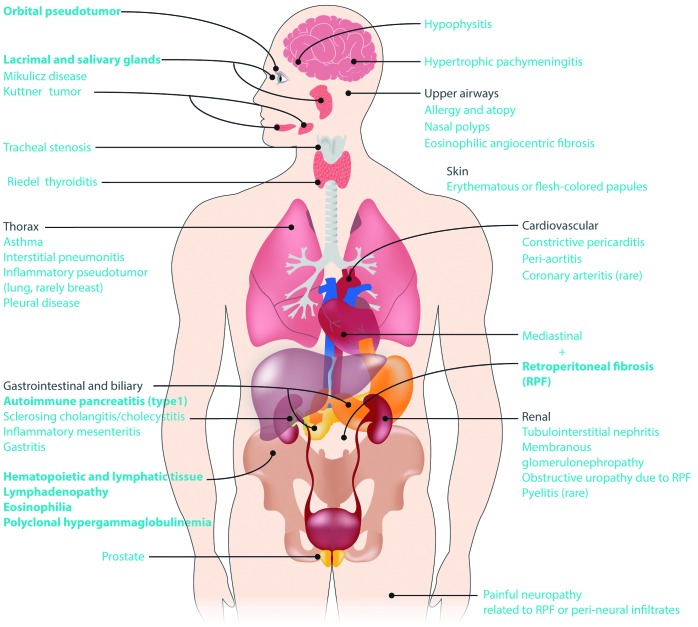
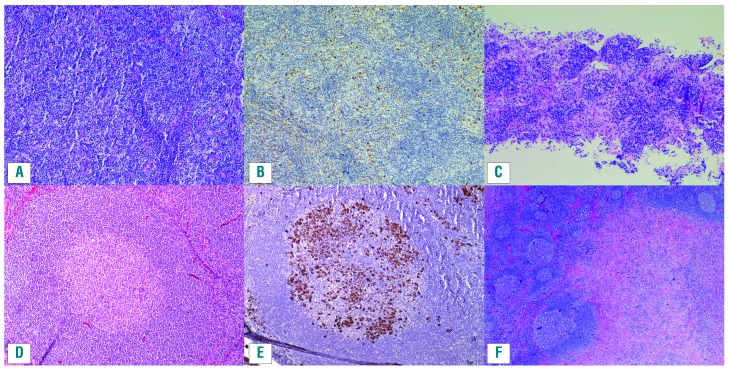
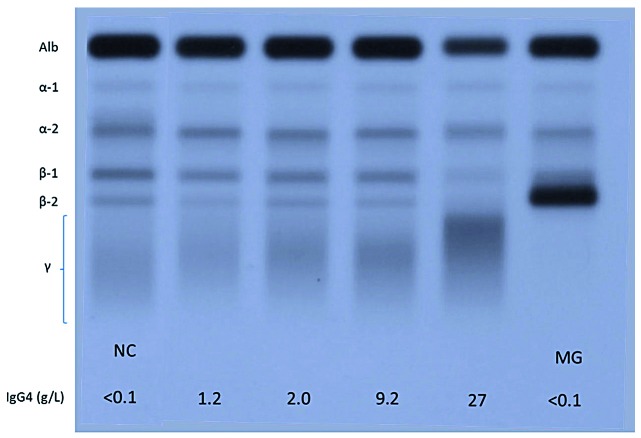
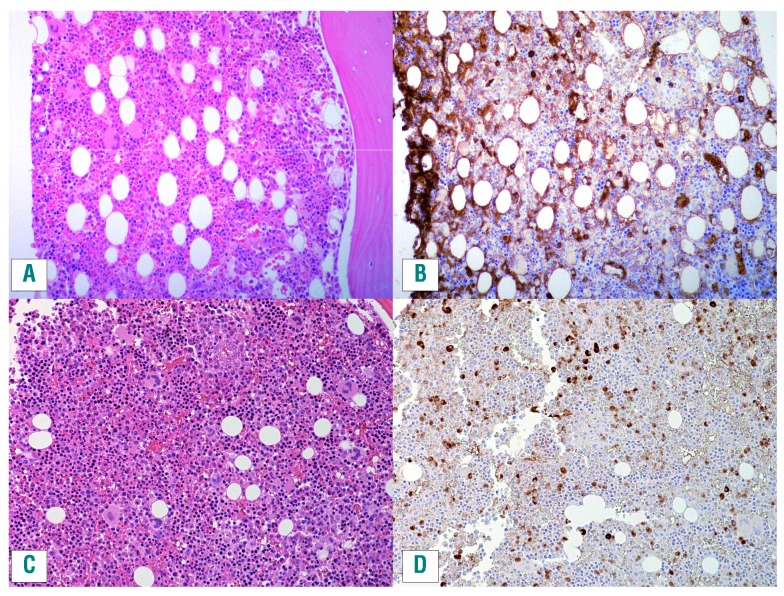
IgG4-related disease is a fibro-inflammatory condition that can affect nearly any organ system. Common presentations include major salivary and lacrimal gland enlargement, orbital disease, autoimmune pancreatitis, retroperitoneal fibrosis and tubulointerstitial nephritis. This review focuses on the hematologic manifestations of IgG4-related disease, including lymphadenopathy, eosinophilia, and polyclonal hypergammaglobulinemia. The disease can easily be missed by unsuspecting hematologists, as patients may present with clinical problems that mimic disorders such as multicentric Castleman disease, lymphoma, plasma cell neoplasms and hypereosinophilic syndromes. When IgG4-related disease is suspected, serum protein electrophoresis and IgG subclasses are helpful as initial tests but a firm histological diagnosis is essential both to confirm the diagnosis and to rule out mimickers. The central histopathological features are a dense, polyclonal, lymphoplasmacytic infiltrate enriched with IgG4-positive plasma cells (with an IgG4/IgG ratio >40%), storiform fibrosis, and obliterative phlebitis. Importantly for hematologists, the latter two features are seen in all tissues except bone marrow and lymph nodes, making these two sites suboptimal for histological confirmation. Many patients follow an indolent course and respond well to treatment, but a significant proportion may have highly morbid or fatal complications such as periaortitis, severe retroperitoneal fibrosis or pachymeningitis. Corticosteroids are effective but cause new or worsening diabetes in about 40% of patients. Initial response rates to rituximab are high but durable remissions are rare. More intensive lymphoma chemotherapy regimens may be required in rare cases of severe, refractory disease, and targeted therapy against plasmablasts, IgE and other disease biomarkers warrant further exploration.
Copyright© 2019 Ferrata Storti Foundation.
Figures
References
-
- Hamano H, Kawa S, Horiuchi A, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732–738. - PubMed
-
- Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol. 2003;38(10):982–984. - PubMed
-
- Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25(9):1181–1192. - PubMed
-
- Mahajan VS, Mattoo H, Deshpande V, Pillai SS, Stone JH. IgG4-related disease. Annu Rev Pathol. 2014;9:315–347. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
