

A pilot, open labelled, randomised controlled trial of hypertonic saline nasal irrigation and gargling for the common cold
- PMID: 30705369
- PMCID: PMC6355924
- DOI: 10.1038/s41598-018-37703-3
A pilot, open labelled, randomised controlled trial of hypertonic saline nasal irrigation and gargling for the common cold
Abstract
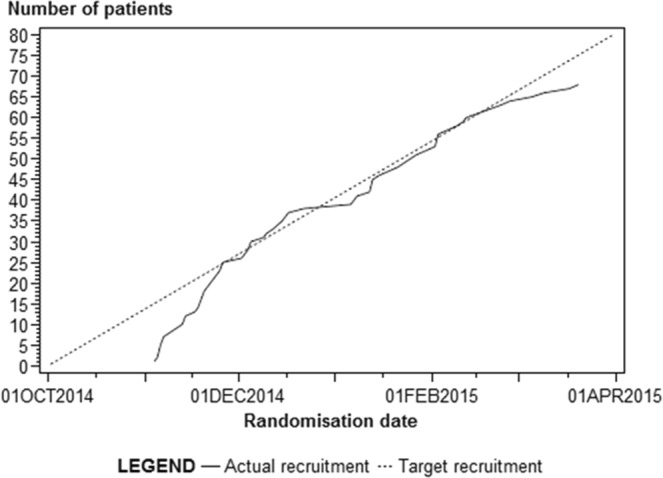
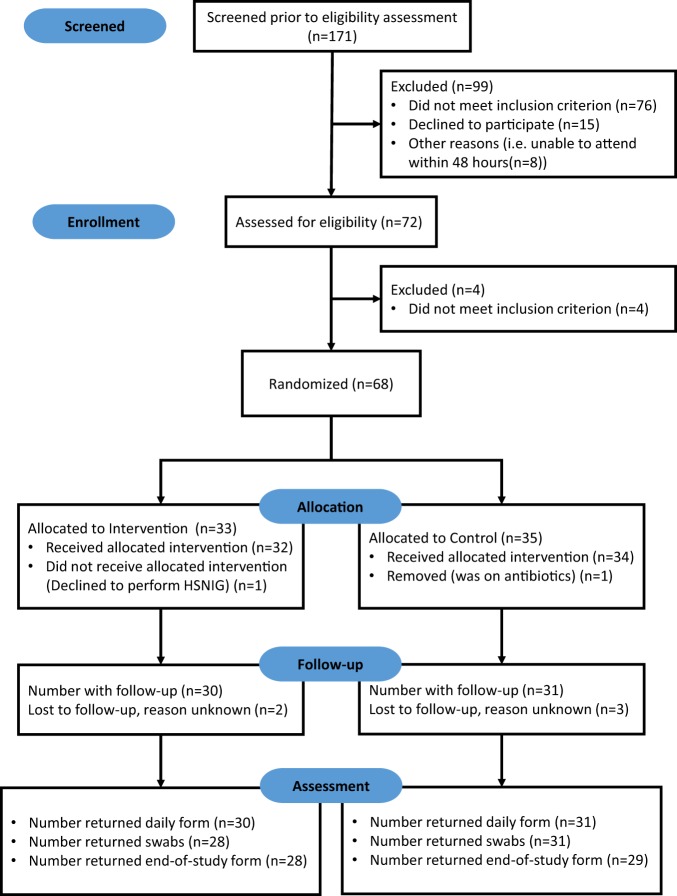
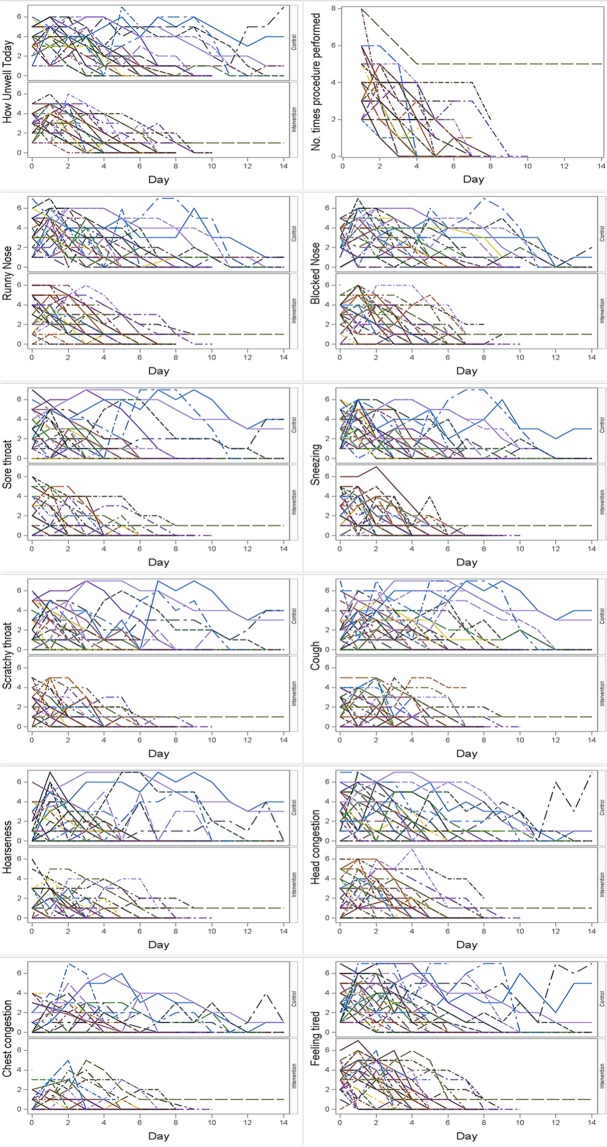
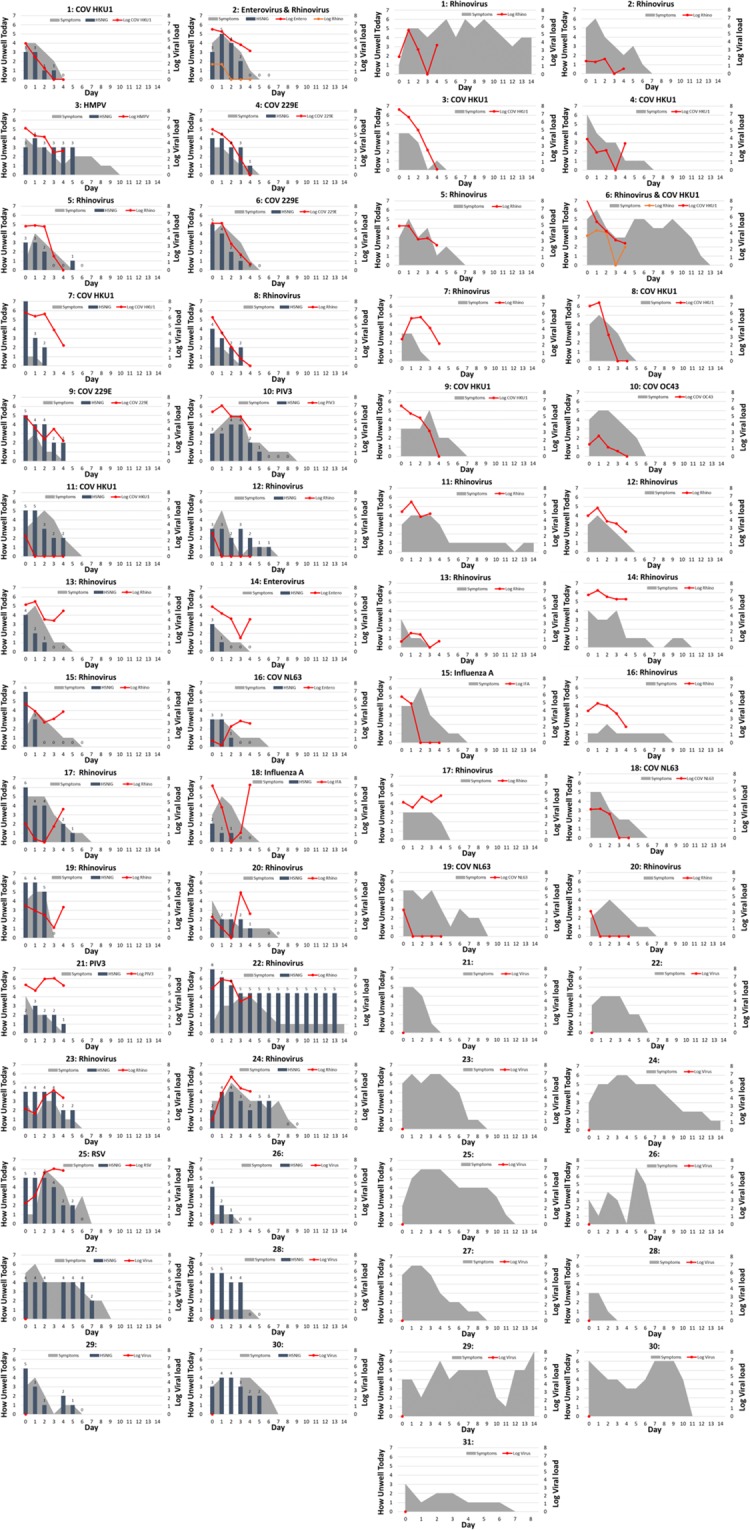
There are no antivirals to treat viral upper respiratory tract infection (URTI). Since numerous viruses cause URTI, antiviral therapy is impractical. As we have evidence of chloride-ion dependent innate antiviral response in epithelial cells, we conducted a pilot, non-blinded, randomised controlled trial of hypertonic saline nasal irrigation and gargling (HSNIG) vs standard care on healthy adults within 48 hours of URTI onset to assess recruitment (primary outcome). Acceptability, symptom duration and viral shedding were secondary outcomes. Participants maintained a symptom diary until well for two days or a maximum of 14 days and collected 5 sequential mid-turbinate swabs to measure viral shedding. The intervention arm prepared hypertonic saline and performed HSNIG. We recruited 68 participants (2.6 participants/week; November 2014-March 2015). A participant declined after randomisation. Another was on antibiotics and hence removed (Intervention:32, Control:34). Follow up data was available from 61 (Intervention:30, Control:31). 87% found HSNIG acceptable, 93% thought HSNIG made a difference to their symptoms. In the intervention arm, duration of illness was lower by 1.9 days (p = 0.01), over-the-counter medications (OTCM) use by 36% (p = 0.004), transmission within household contacts by 35% (p = 0.006) and viral shedding by ≥0.5 log10/day (p = 0.04). We hence need a larger trial to confirm our findings.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Efficacy and safety of a hypertonic seawater nasal irrigation solution containing algal and herbal natural ingredients in patients with COVID-19.Eur Rev Med Pharmacol Sci. 2022 Dec;26(2 Suppl):112-123. doi: 10.26355/eurrev_202212_30495. Eur Rev Med Pharmacol Sci. 2022. PMID: 36524919
References
-
- Office for National Statistics: Sickness absence in the labour market: 2016. (London, 2017).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
