

Changes in Cognition, Depression and Quality of Life after Carotid Stenosis Treatment
- PMID: 30706811
- PMCID: PMC6696820
- DOI: 10.2174/1567202616666190129153409
Changes in Cognition, Depression and Quality of Life after Carotid Stenosis Treatment
Abstract
Background: Although several studies have evaluated the change of cognitive performance after severe carotid artery stenosis, the results still remain elusive. The objective of this study was to assess changes in cognitive function, depressive symptoms and Health Related Quality of Life (HRQoL) after carotid stenosis revascularisation and Best Medical Treatment (BMT).
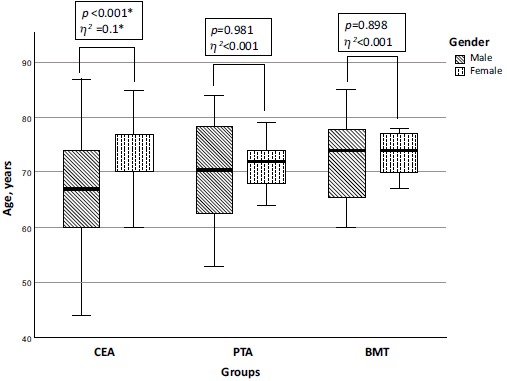
Methods: Study involved 213 patients with ≥70% carotid stenosis who underwent assessment of cognitive function using Montreal Cognitive Assessment scale (MoCA), depressive symptoms - using Patient Health Questionnaire-9 (PHQ-9) and HRQoL - using Medical Outcome Survey Short Form version 2 (SF-36v2). The assessment was performed before and at 6 and 12 months followup periods in patients who had Carotid Endarterectomy (CEA), Carotid Artery Stenting (CAS) or received BMT only.
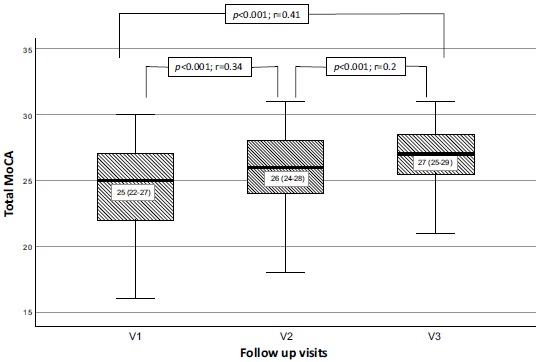
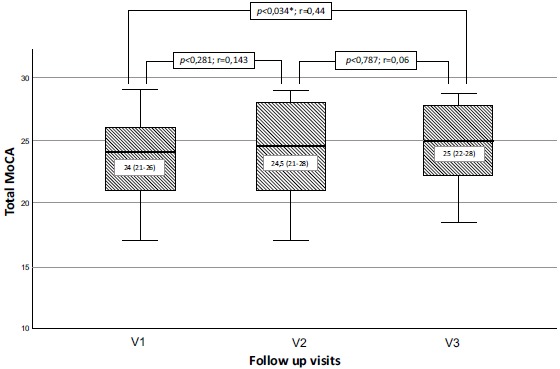
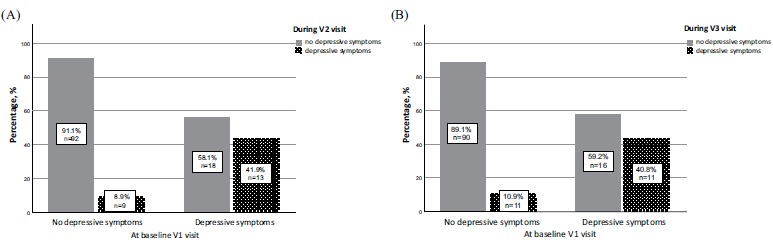
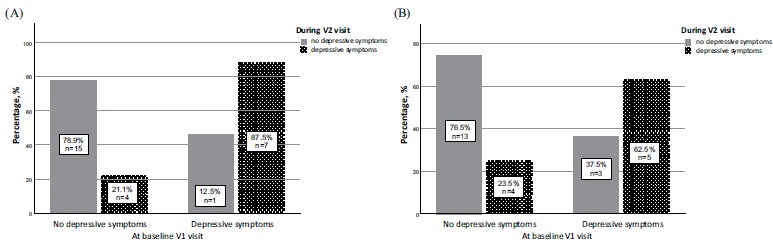
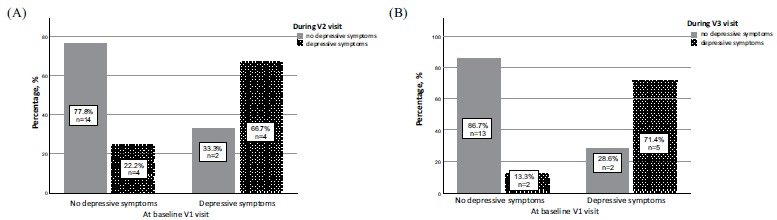
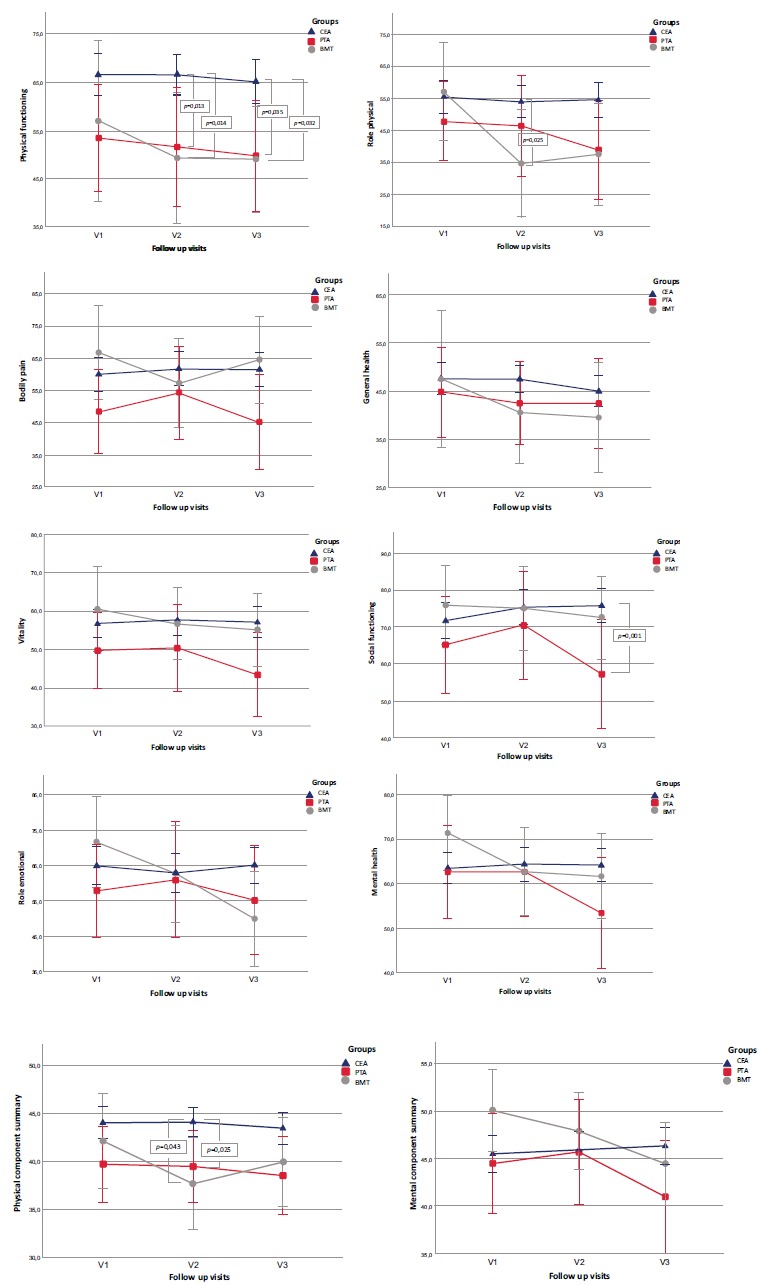
Results: Improvement in the total MoCA scores was observed after 6 and 12 months (p<0.001, Kendall's W=0.28) in the CEA group. In the CAS group - after 12 months (p=0.01, Kendall's W=0.261) whereas in the BMT group - no significant changes (p=0.295, Kendall's W=0.081) were observed. Reduction of depressive symptoms was not found in any of the study groups. Comparing mean SF-36v2 scores in the CEA group, there was no significant difference in any of 10 subscales. Likewise in the CAS group - no significant difference in 9 of 10 subscales (p=0.028, η2=0.343) was observed. Three subscales worsened in the BMT group during the 1-year follow-up period.
Conclusion: Patients with severe carotid stenosis who underwent revascularisation enhanced their cognitive performance without exerting significant change of depressive symptoms. Preoperative HRQoL may be maintained for at least one year in the CEA group.
Keywords: Cognition; carotid stenosis; depression; endarterectomy; medical treatment; quality of life; stenting..
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
Similar articles
-
Improvement of cognitive function after carotid endarterectomy--a new strategy for the evaluation of cognitive function.J Stroke Cerebrovasc Dis. 2014 Jul;23(6):1332-6. doi: 10.1016/j.jstrokecerebrovasdis.2013.11.004. Epub 2014 Jan 22. J Stroke Cerebrovasc Dis. 2014. PMID: 24462461
-
Cognitive Change 1 Year after CEA or CAS Compared with Medication.J Stroke Cerebrovasc Dis. 2017 Jun;26(6):1297-1305. doi: 10.1016/j.jstrokecerebrovasdis.2017.01.024. Epub 2017 Feb 22. J Stroke Cerebrovasc Dis. 2017. PMID: 28236597
-
Carotid Endarterectomy and Carotid Artery Stenting Lead to Improved Cognitive Performance in Patients with Severe Carotid Artery Stenosis.Curr Neurovasc Res. 2016;13(1):45-9. doi: 10.2174/1567202613666151116143757. Curr Neurovasc Res. 2016. PMID: 26666638
-
Effects of Carotid Artery Stent and Carotid Endarterectomy on Cognitive Function in Patients with Carotid Stenosis.Biomed Res Int. 2020 Dec 16;2020:6634537. doi: 10.1155/2020/6634537. eCollection 2020. Biomed Res Int. 2020. Retraction in: Biomed Res Int. 2024 Mar 20;2024:9806516. doi: 10.1155/2024/9806516. PMID: 33381568 Free PMC article. Retracted. Review.
-
The impact of carotid artery stenting on cognitive function in patients with extracranial carotid artery stenosis.Ann Vasc Surg. 2015 Apr;29(3):457-69. doi: 10.1016/j.avsg.2014.10.024. Epub 2015 Jan 13. Ann Vasc Surg. 2015. PMID: 25591487 Review.
Cited by
-
Cognitive Functions in Patients after Carotid Artery Revascularization-A Narrative Review.Brain Sci. 2021 Oct 1;11(10):1307. doi: 10.3390/brainsci11101307. Brain Sci. 2021. PMID: 34679372 Free PMC article. Review.
-
Early Age of Migraine Onset is Independently Related to Cognitive Decline and Symptoms of Depression Affect Quality of Life.Curr Neurovasc Res. 2020;17(2):177-187. doi: 10.2174/1567202617666200207130659. Curr Neurovasc Res. 2020. PMID: 32031072 Free PMC article.
-
Cognitive impairment and quality of life among patients with carotid artery stenosis in Jordan: a cross-sectional study.Sci Rep. 2025 Jun 4;15(1):19639. doi: 10.1038/s41598-025-04004-5. Sci Rep. 2025. PMID: 40467666 Free PMC article.
-
Cognitive effects of carotid revascularization in octogenarians.Surgery. 2023 Oct;174(4):1078-1082. doi: 10.1016/j.surg.2023.07.010. Epub 2023 Aug 6. Surgery. 2023. PMID: 37550167 Free PMC article.
-
Differential Cognitive Functioning and Benefit From Surgery in Patients Undergoing Coronary Artery Bypass Grafting and Carotid Endarterectomy.Front Neurol. 2022 Mar 8;13:824486. doi: 10.3389/fneur.2022.824486. eCollection 2022. Front Neurol. 2022. PMID: 35350398 Free PMC article.
References
-
- Naylor A.R. Why is the management of asymptomatic carotid disease so controversial? Surgeon. 2015;13(1):34–43. - PubMed
-
- Hackett M.L., Pickles K., Part I. Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke. 2014;9(8):1017–1025. - PubMed
-
- Wang T., Mei B., Zhang J. Atherosclerotic carotid stenosis and cognitive function. Clin. Neurol. Neurosurg. 2016;146:64–70. - PubMed
-
- Lal B.K., Dux M.C., Sikdar S., et al. Asymptomatic carotid stenosis is associated with cognitive impairment. J. Vasc. Surg. 2017;66(4):1083–1092. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
