

Early-onset Alzheimer Disease and Its Variants
- PMID: 30707186
- PMCID: PMC6538053
- DOI: 10.1212/CON.0000000000000687
Early-onset Alzheimer Disease and Its Variants
Abstract
Purpose of review: Early-onset Alzheimer disease (AD) is defined as having an age of onset younger than 65 years. While early-onset AD is often overshadowed by the more common late-onset AD, recognition of the differences between early- and late-onset AD is important for clinicians.
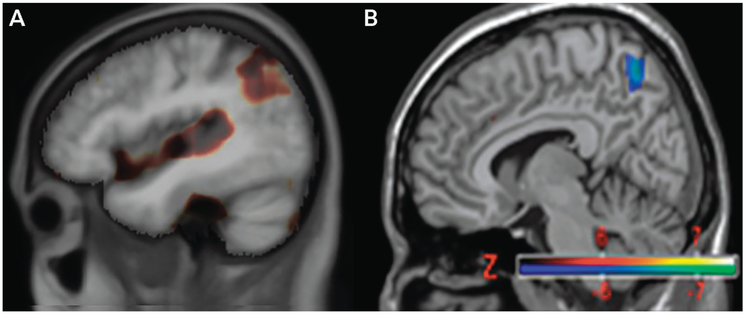
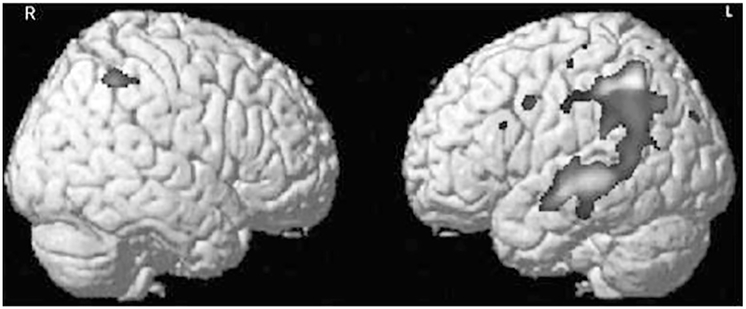
Recent findings: Early-onset AD comprises about 5% to 6% of cases of AD and includes a substantial percentage of phenotypic variants that differ from the usual amnestic presentation of typical AD. Characteristics of early-onset AD in comparison to late-onset AD include a larger genetic predisposition (familial mutations and summed polygenic risk), more aggressive course, more frequent delay in diagnosis, higher prevalence of traumatic brain injury, less memory impairment and greater involvement of other cognitive domains on presentation, and greater psychosocial difficulties. Neuroimaging features of early-onset AD in comparison to late-onset AD include greater frequency of hippocampal sparing and posterior neocortical atrophy, increased tau burden, and greater connectomic changes affecting frontoparietal networks rather than the default mode network.
Summary: Early-onset AD differs substantially from late-onset AD, with different phenotypic presentations, greater genetic predisposition, and differences in neuropathologic burden and topography. Early-onset AD more often presents with nonamnestic phenotypic variants that spare the hippocampi and with greater tau burden in posterior neocortices. The early-onset AD phenotypic variants involve different neural networks than typical AD. The management of early-onset AD is similar to that of late-onset AD but with special emphasis on targeting specific cognitive areas and more age-appropriate psychosocial support and education.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical