

Prevention of Prescription Opioid Misuse and Projected Overdose Deaths in the United States
- PMID: 30707224
- PMCID: PMC6415966
- DOI: 10.1001/jamanetworkopen.2018.7621
Prevention of Prescription Opioid Misuse and Projected Overdose Deaths in the United States
Abstract
Importance: Deaths due to opioid overdose have tripled in the last decade. Efforts to curb this trend have focused on restricting the prescription opioid supply; however, the near-term effects of such efforts are unknown.
Objective: To project effects of interventions to lower prescription opioid misuse on opioid overdose deaths from 2016 to 2025.
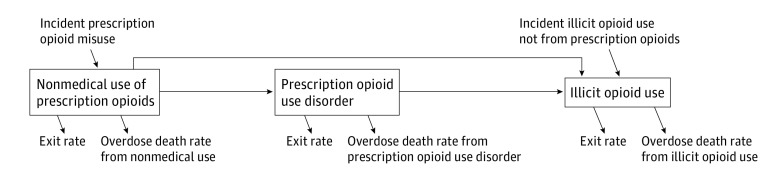
Design, setting, and participants: This system dynamics (mathematical) model of the US opioid epidemic projected outcomes of simulated individuals who engage in nonmedical prescription or illicit opioid use from 2016 to 2025. The analysis was performed in 2018 by retrospectively calibrating the model from 2002 to 2015 data from the National Survey on Drug Use and Health and the Centers for Disease Control and Prevention.
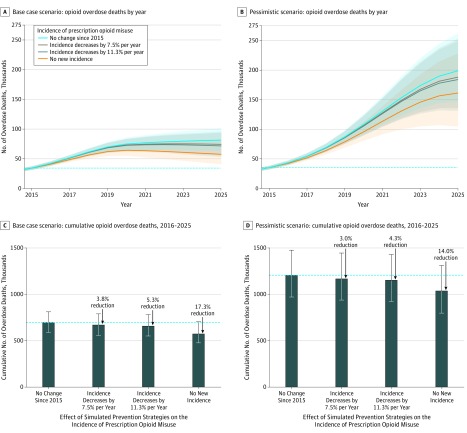
Interventions: Comparison of interventions that would lower the incidence of prescription opioid misuse from 2016 to 2025 based on historical trends (a 7.5% reduction per year) and 50% faster than historical trends (an 11.3% reduction per year), vs a circumstance in which the incidence of misuse remained constant after 2015.
Main outcomes and measures: Opioid overdose deaths from prescription and illicit opioids from 2016 to 2025 under each intervention.
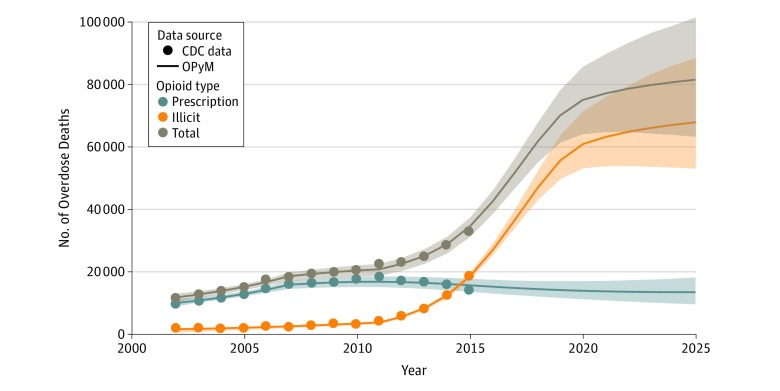
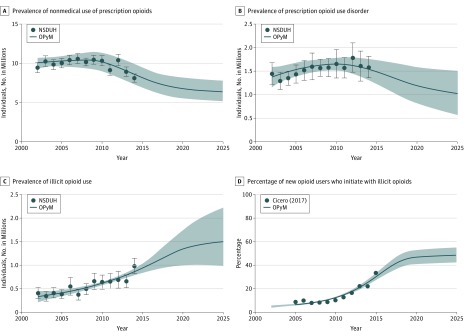
Results: Under the status quo, the annual number of opioid overdose deaths is projected to increase from 33 100 in 2015 to 81 700 (95% uncertainty interval [UI], 63 600-101 700) in 2025 (a 147% increase from 2015). From 2016 to 2025, 700 400 (95% UI, 590 200-817 100) individuals in the United States are projected to die from opioid overdose, with 80% of the deaths attributable to illicit opioids. The number of individuals using illicit opioids is projected to increase by 61%-from 0.93 million (95% UI, 0.83-1.03 million) in 2015 to 1.50 million (95% UI, 0.98-2.22 million) by 2025. Across all interventions tested, further lowering the incidence of prescription opioid misuse from 2015 levels is projected to decrease overdose deaths by only 3.0% to 5.3%.
Conclusions and relevance: This study's findings suggest that interventions targeting prescription opioid misuse such as prescription monitoring programs may have a modest effect, at best, on the number of opioid overdose deaths in the near future. Additional policy interventions are urgently needed to change the course of the epidemic.
Conflict of interest statement
Figures
References
-
- CDC WONDER Multiple cause of death 1999-2017. https://wonder.cdc.gov/controller/datarequest/D77. Accessed June 29, 2017.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
