

Prediction of high nodal burden with ultrasound and magnetic resonance imaging in clinically node-negative breast cancer patients
- PMID: 30709369
- PMCID: PMC6359788
- DOI: 10.1186/s40644-019-0191-y
Prediction of high nodal burden with ultrasound and magnetic resonance imaging in clinically node-negative breast cancer patients
Abstract
Background: Although the role of axillary imaging has been redirected for predicting high nodal burden rather than predicting nodal metastases since ACOSOG Z1011 trial, it remains unclear whether and how axillary lymph node (ALN) characteristics predicts high nodal burden. Our study was aimed to evaluate the predictive value of imaging characteristics of ALNs at ultrasound and magnetic resonance imaging (MRI) for prediction of high nodal burden (≥3 metastatic ALNs) in clinically node-negative breast cancer patients.
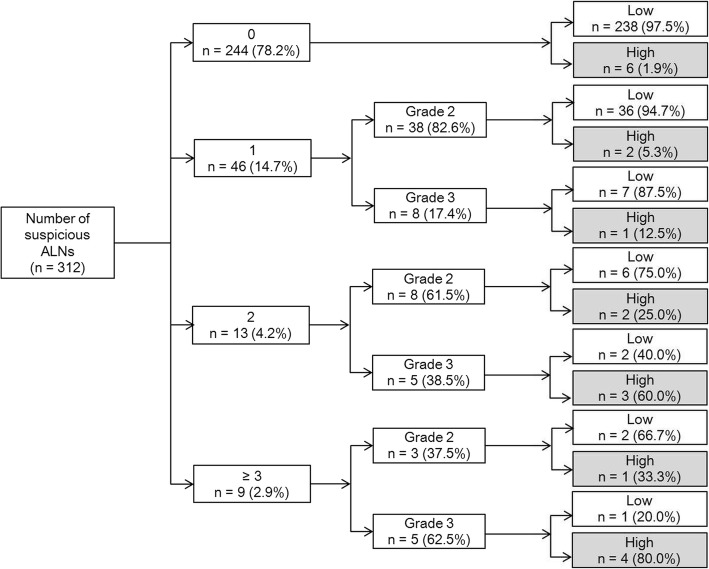
Methods: Clinicopathological and imaging characteristics were evaluated in patients with ultrasound (n = 312) and MRI (n = 256). Imaging characteristics include number of suspicious ALNs and cortical morphologic changes (grade 1, cortical thickness < 2 mm; grade 2, 2-5 mm; grade 3, ≥5 mm or fatty hilum loss). Odds ratios (ORs) were calculated using multivariate analysis.
Results: For ultrasound, higher (≥2) T stage (OR = 5.65, P = .005), higher number of suspicious ALNs (2 suspicious ALNs, OR = 6.52, P = .019; ≥ 3 suspicious ALNs, OR = 21.08, P = .005), and grade 3 of cortical morphologic changes (OR = 9.85, P = .023) independently associated with high nodal burden. For MRI, higher (≥2) T stage (OR = 5.17, P = .011) and higher number of suspicious ALNs (2 suspicious ALNs, OR = 69.00, P = .001; ≥ 3 suspicious ALNs, OR = 93.55, P < .001) were independently associated with high nodal burden. Among patients with 2 suspicious ALNs, those with grade 3 cortical morphologic change at ultrasound had a higher rate of high nodal burden than those with grade 2 (60.0% [3/5] vs. 25.0% [2/8]).
Conclusions: A higher number of suspicious ALNs is an independent predictor for high nodal burden. Further stratification can be achieved by incorporating assessment of ultrasound-based cortical morphologic changes.
Keywords: Axilla; Axillary nodes; Breast cancer; Lymph nodes; Magnetic resonance imaging; Ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Due to our retrospective review of prospectively collected data, and the requirement of an informed consent was waived after approval of institutional review board.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Combining the Ultrasound Features of Primary Tumor and Axillary Lymph Nodes Can Reduce False-Negative Rate during the Prediction of High Axillary Node Burden in BI-RADS Category 4 or 5 Breast Cancer Lesions.Ultrasound Med Biol. 2020 Aug;46(8):1941-1948. doi: 10.1016/j.ultrasmedbio.2020.04.003. Epub 2020 May 22. Ultrasound Med Biol. 2020. PMID: 32451195
-
Preoperative axillary nodal staging with ultrasound and magnetic resonance imaging: predictive values of quantitative and semantic features.Br J Radiol. 2018 Dec;91(1092):20180507. doi: 10.1259/bjr.20180507. Epub 2018 Aug 29. Br J Radiol. 2018. PMID: 30059242 Free PMC article.
-
Ultrasound-Guided Fine-Needle Aspiration of Non-palpable and Suspicious Axillary Lymph Nodes with Subsequent Removal after Tattooing: False-Negative Results and Concordance with Sentinel Lymph Nodes.Ultrasound Med Biol. 2017 Nov;43(11):2576-2581. doi: 10.1016/j.ultrasmedbio.2017.07.011. Epub 2017 Aug 19. Ultrasound Med Biol. 2017. PMID: 28830644
-
Sonographic localisation of lymph nodes suspicious of metastatic breast cancer to surgical axillary levels.J Med Radiat Sci. 2025 Mar;72(1):119-138. doi: 10.1002/jmrs.840. Epub 2024 Nov 17. J Med Radiat Sci. 2025. PMID: 39552171 Free PMC article. Review.
-
Role of sonography for the locoregional staging of breast cancer.AJR Am J Roentgenol. 2014 Nov;203(5):1132-41. doi: 10.2214/AJR.13.12311. AJR Am J Roentgenol. 2014. PMID: 25341155 Review.
Cited by
-
Mode of presentation and skin thickening on ultrasound may predict nodal burden in breast cancer patients with a positive axillary core biopsy.Br J Radiol. 2020 Apr;93(1108):20190711. doi: 10.1259/bjr.20190711. Epub 2020 Jan 28. Br J Radiol. 2020. PMID: 31971817 Free PMC article.
-
Prediction of axillary nodal burden using preoperative magnetic resonance imaging scoring in patients with clinically node-negative breast cancer: a retrospective cohort study.Gland Surg. 2024 Dec 31;13(12):2288-2299. doi: 10.21037/gs-24-379. Epub 2024 Dec 27. Gland Surg. 2024. PMID: 39822365 Free PMC article.
-
Automated Versus Handheld Breast Ultrasound for Evaluating Axillary Lymph Nodes in Patients With Breast Cancer.Korean J Radiol. 2024 Feb;25(2):146-156. doi: 10.3348/kjr.2023.0100. Epub 2024 Jan 17. Korean J Radiol. 2024. PMID: 38238017 Free PMC article.
-
Radiomics Analysis of Contrast-Enhanced Breast MRI for Optimized Modelling of Virtual Prognostic Biomarkers in Breast Cancer.Eur J Breast Health. 2024 Apr 1;20(2):122-128. doi: 10.4274/ejbh.galenos.2024.2023-12-12. eCollection 2024 Apr. Eur J Breast Health. 2024. PMID: 38571687 Free PMC article.
-
Prediction of axillary nodal burden in patients with invasive lobular carcinoma using MRI.Breast Cancer Res Treat. 2021 Apr;186(2):463-473. doi: 10.1007/s10549-020-06056-9. Epub 2021 Jan 3. Breast Cancer Res Treat. 2021. PMID: 33389406
References
-
- Galimberti V, Cole BF, Zurrida S, Viale G, Luini A, Veronesi P, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 2013;14:297–305. doi: 10.1016/S1470-2045(13)70035-4. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
