

Prediction Model for Nodal Disease Among Patients With Non-Small Cell Lung Cancer
- PMID: 30710518
- PMCID: PMC6535349
- DOI: 10.1016/j.athoracsur.2018.12.041
Prediction Model for Nodal Disease Among Patients With Non-Small Cell Lung Cancer
Abstract
Background: We characterized the performance characteristics of guideline-recommended invasive mediastinal staging (IMS) for lung cancer and developed a prediction model for nodal disease as a potential alternative approach to staging.
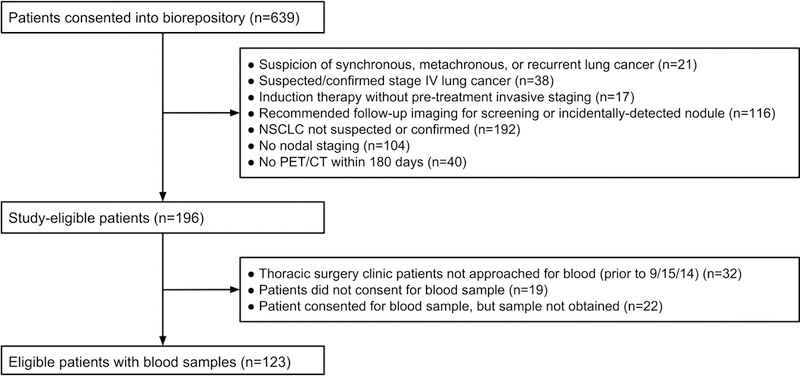
Methods: We conducted a prospective cohort study of adults with suspected/confirmed non-small cell lung cancer without evidence of distant metastatic disease (by computed tomography/positron emission tomography) who underwent nodal evaluation by IMS and/or at the time of resection. The true-positive rate was the proportion of patients with true nodal disease selected to undergo IMS based on guideline recommendations, and the false-positive rate was the proportion of patients without true nodal disease selected to undergo IMS. Logistic regression was used to predict nodal disease using radiographic predictors.
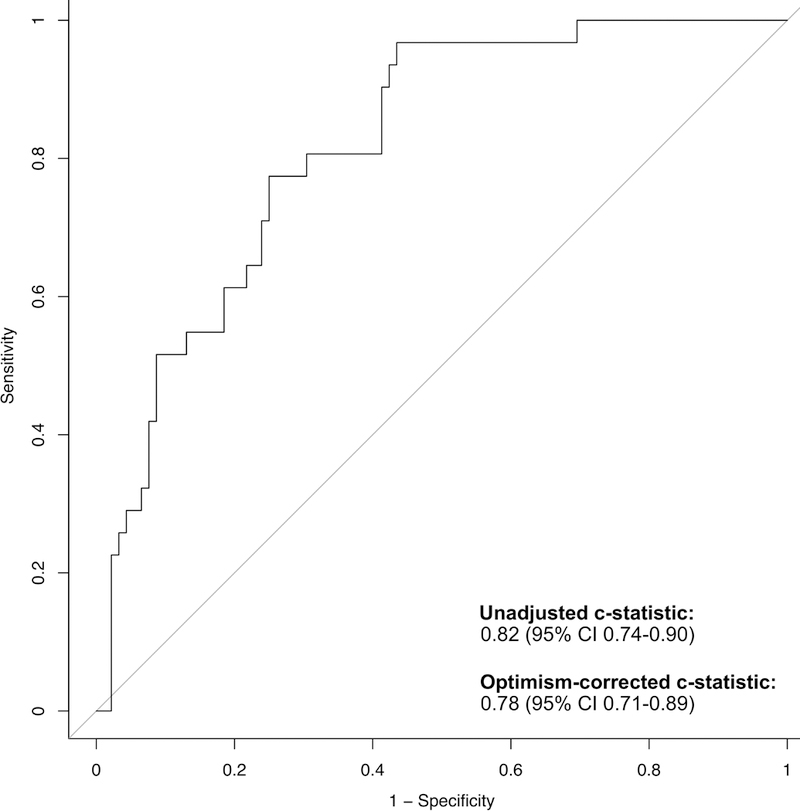
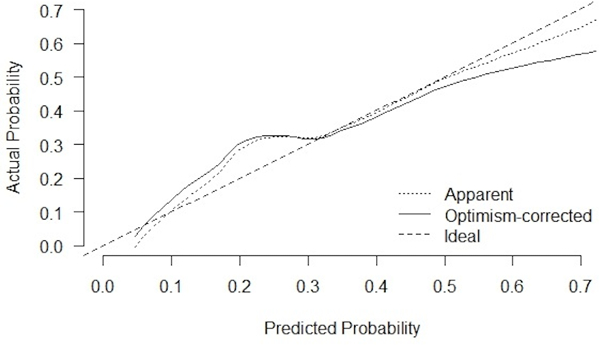
Results: Among 123 eligible subjects, 31 (25%) had pathologically confirmed nodal disease. A guideline-recommended invasive staging strategy had a true-positive rate and false-positive rate of 100% and 65%, respectively. The prediction model fit the data well (goodness-of-fit test, p = 0.55) and had excellent discrimination (optimism corrected c-statistic, 0.78; 95% confidence interval, 0.72 to 0.89). Exploratory analysis revealed that use of the prediction model could achieve a false-positive rate of 44% and a true-positive rate of 97%.
Conclusions: A guideline-recommended strategy for IMS selects all patients with true nodal disease and most patients without nodal disease for IMS. Our prediction model appears to maintain (within a margin of error) the sensitivity of a guideline-recommended invasive staging strategy and has the potential to reduce the use of invasive procedures.
Copyright © 2019 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Presented at the CHEST® annual meeting in Toronto, Canada November 1, 2017.
Figures
Comment in
-
The importance of the false-negative rate to validate a staging protocol for non-small cell lung cancer.Transl Lung Cancer Res. 2019 Dec;8(Suppl 4):S400-S402. doi: 10.21037/tlcr.2019.07.04. Transl Lung Cancer Res. 2019. PMID: 32038924 Free PMC article. No abstract available.
-
Methodological Issue in Prediction Model for Nodal Disease Among Patients With Lung Cancer.Ann Thorac Surg. 2020 Aug;110(2):747. doi: 10.1016/j.athoracsur.2020.01.008. Epub 2020 Feb 18. Ann Thorac Surg. 2020. PMID: 32084374 No abstract available.
-
A Prediction Model for Nodal Disease: Practical Considerations in the Evaluation of Model Performance: Reply.Ann Thorac Surg. 2020 Aug;110(2):747. doi: 10.1016/j.athoracsur.2020.03.054. Epub 2020 Apr 23. Ann Thorac Surg. 2020. PMID: 32335019 No abstract available.
References
-
- Porter ME. What is value in health care. N Engl J Med. 2010;363(26):2477–2481. - PubMed
-
- Silvestri GA, Gonzalez AV, Jantz MA, et al. Methods for Staging Non-small Cell Lung Cancer. Chest. 2013;143(5):e211S–e250S. - PubMed
-
- National Comprehensive Cancer Network. Clinical practice guidelines in oncology v.4.2016: Non-small cell lung cancer. NCCN Guidel. 2016. - PubMed
-
- Lemaire A, Nikolic I, Petersen T, et al. Nine-Year Single Center Experience With Cervical Mediastinoscopy: Complications and False Negative Rate. Ann Thorac Surg. 2006;82(4):1185–1190. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
