

Anatomical features of primary brain tumors affect seizure risk and semiology
- PMID: 30710869
- PMCID: PMC6354289
- DOI: 10.1016/j.nicl.2019.101688
Anatomical features of primary brain tumors affect seizure risk and semiology
Abstract
Objective: An epileptic seizure is the most common clinical manifestation of a primary brain tumor. Due to modern neuroimaging, detailed anatomical information on a brain tumor is available early in the diagnostic process and therefore carries considerable potential in clinical decision making. The goal of this study was to gain a better understanding of the relevance of anatomical tumor characteristics on seizure prevalence and semiology.
Methods: We reviewed prospectively collected clinical and imaging data of all patients operated on a supratentorial intraparenchymal primary brain tumor at our department between January 2009 and December 2016. The effect of tumor histology, anatomical location and white matter infiltration on seizure prevalence and semiology were assessed using uni- and multivariate analyses.
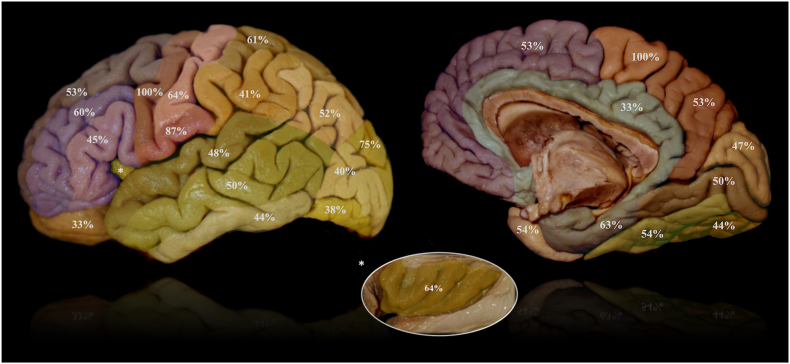
Results: Of 678 included patients, 311 (45.9%) presented with epileptic seizures. Tumor location within the central lobe was associated with higher seizure prevalence (OR 4.67, 95% CI: 1.90-13.3, p = .002), especially within the precentral gyrus or paracentral lobule (100%). Bilateral extension, location within subcortical structures and invasion of deeper white matter sectors were associated with a lower risk (OR 0.45, 95% CI: 0.25-0.78; OR 0.10, 95% CI: 0.04-0.21 and OR 0.39, 95% CI: 0.14-0.96, respectively). Multivariate analysis revealed the impact of a location within the central lobe on seizure risk to be highly significant and more relevant than histopathology (OR: 4.79, 95% CI: 1.82-14.52, p = .003). Seizures due to tumors within the central lobe differed from those of other locations by lower risk of secondary generalization (p < .001).
Conclusions: Topographical lobar and gyral location, as well as extent of white matter infiltration impact seizure risk and semiology. This finding may have a high therapeutic potential, for example regarding the use of prophylactic antiepileptic therapy.
Keywords: Anatomy; Brain tumor; Central lobe; Epilepsy; Glioma; Histology; Seizures; Topography; White matter sectors.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Figures





References
-
- Brodmann K. Barth; Leipzig: 1909. Vergleichende Lokalisationslehre der Grosshirnrinde in ihren Prinzipien dargestellt auf Grund des Zellenbaues; pp. 1–324.
-
- Chang E.F., Potts M.B., Keles G.E., Lamborn K.R., Chang S.M., Barbaro N.M., Berger M.S. Seizure characteristics and control following resection in 332 patients with low-grade gliomas. J. Neurosurg. 2008;108:227–235. - PubMed
-
- Chouinard P.A., Paus T. The primary motor and premotor areas of the human cerebral cortex. Neuroscience. 2006;12:143–152. - PubMed
-
- Collins R.C., Dobkin B.H., Choi D.W. Selective vulnerability of the brain: new insights into the pathophysiology of stroke. Ann. Intern. Med. 1989;110(12):992–1000. - PubMed
-
- Dalmau J., Graus F. Antibody-mediated encephalitis. N. Engl. J. Med. 2018;378:840–851. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
