

Automated segmentation of haematoma and perihaematomal oedema in MRI of acute spontaneous intracerebral haemorrhage
- PMID: 30711800
- PMCID: PMC6382492
- DOI: 10.1016/j.compbiomed.2019.01.022
Automated segmentation of haematoma and perihaematomal oedema in MRI of acute spontaneous intracerebral haemorrhage
Abstract
Background: Spontaneous intracerebral haemorrhage (SICH) is a common condition with high morbidity and mortality. Segmentation of haematoma and perihaematoma oedema on medical images provides quantitative outcome measures for clinical trials and may provide important markers of prognosis in people with SICH.
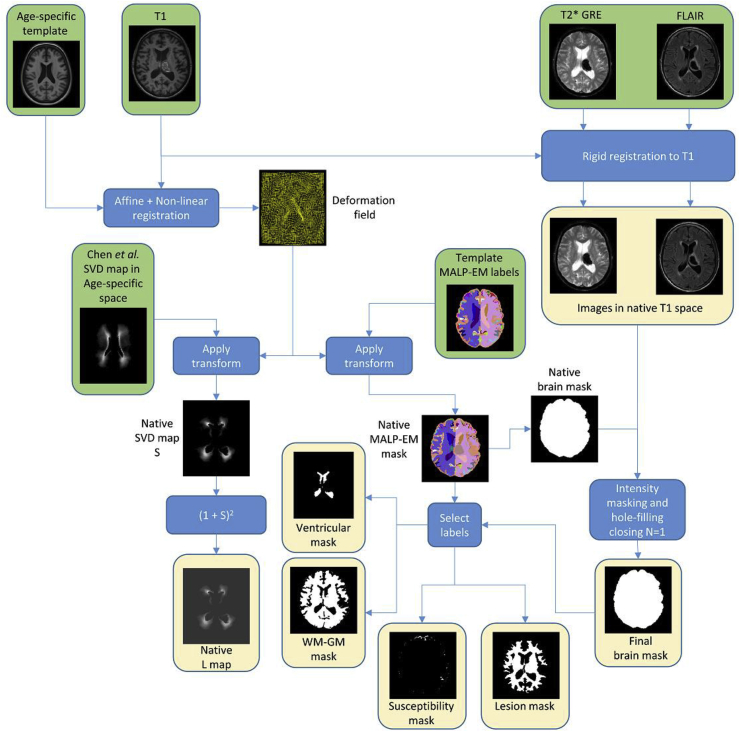
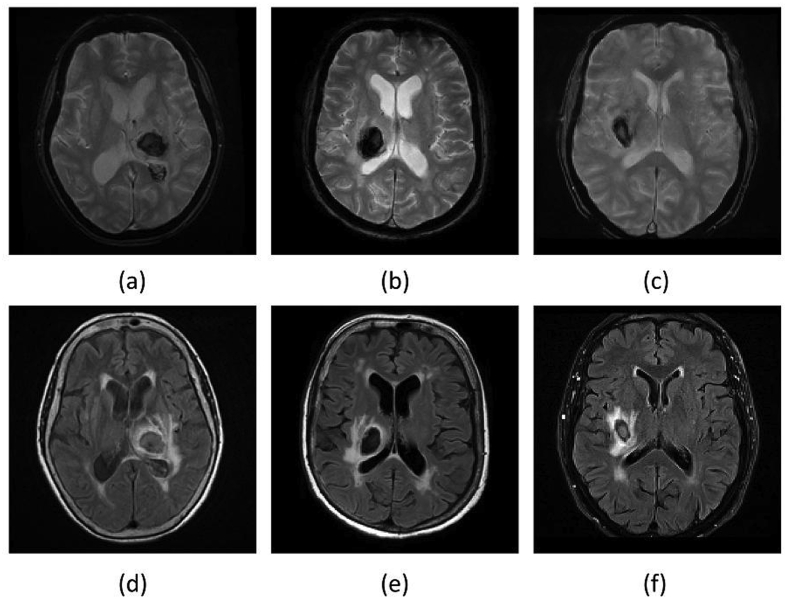
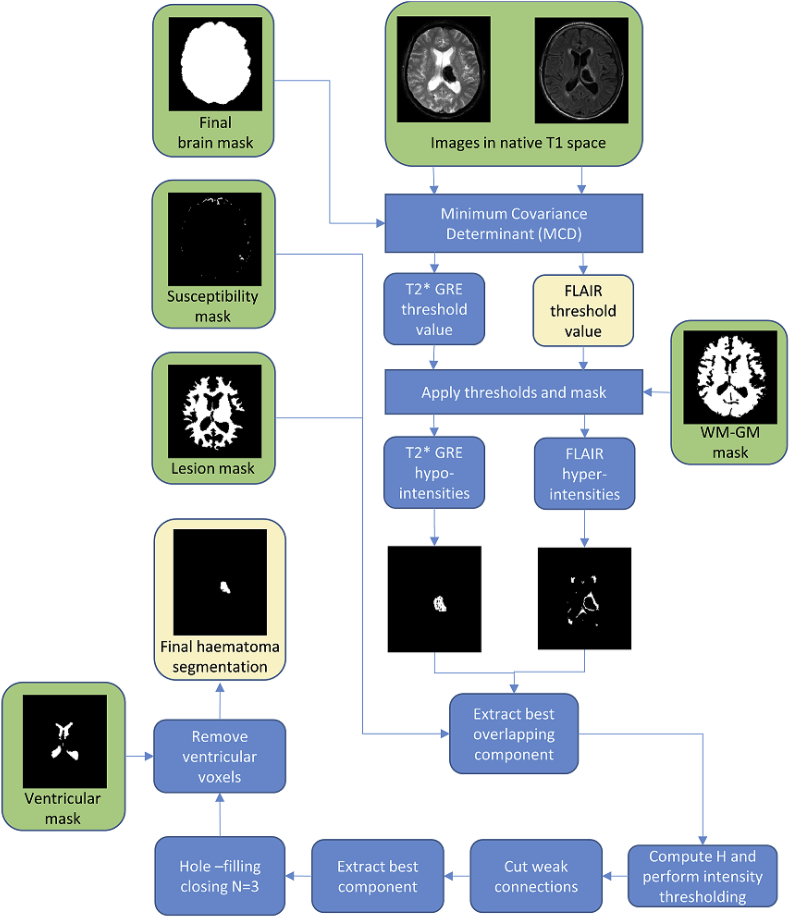
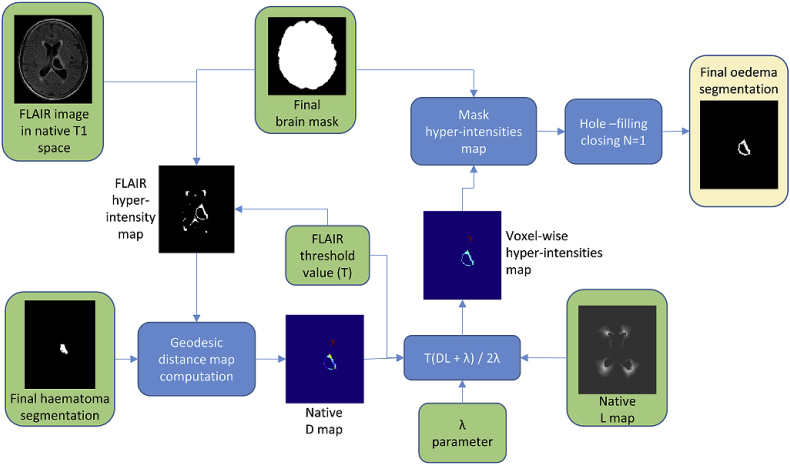
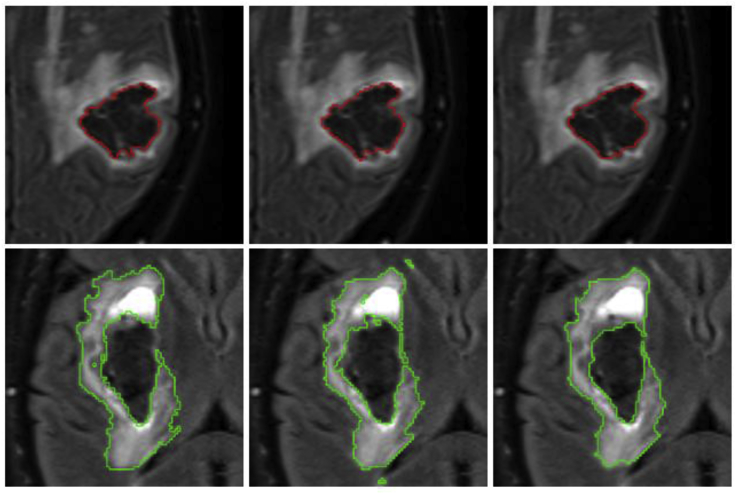
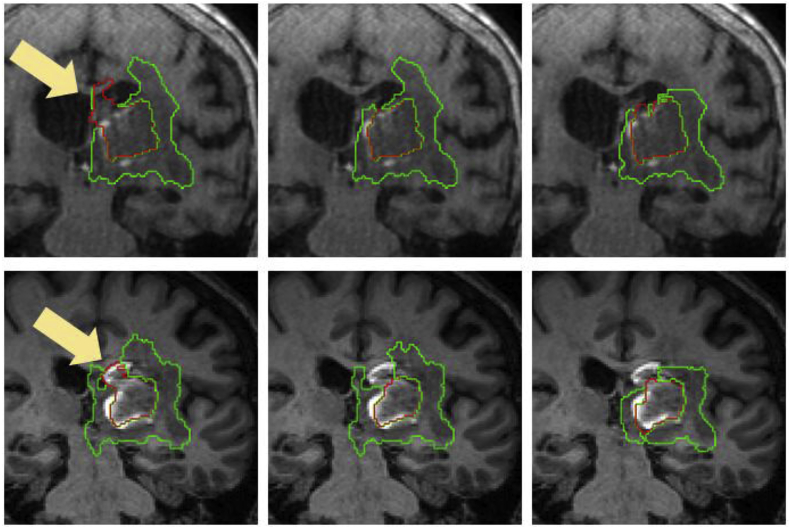
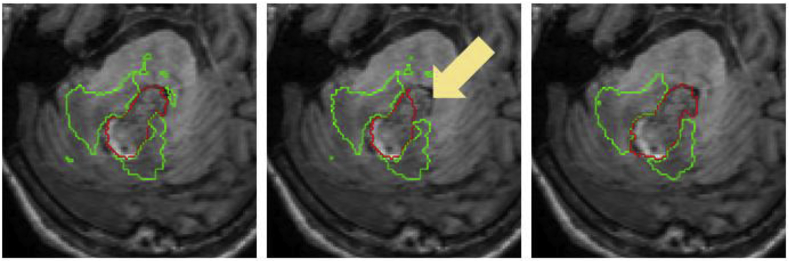
Methods: We take advantage of improved contrast seen on magnetic resonance (MR) images of patients with acute and early subacute SICH and introduce an automated algorithm for haematoma and oedema segmentation from these images. To our knowledge, there is no previously proposed segmentation technique for SICH that utilises MR images directly. The method is based on shape and intensity analysis for haematoma segmentation and voxel-wise dynamic thresholding of hyper-intensities for oedema segmentation.
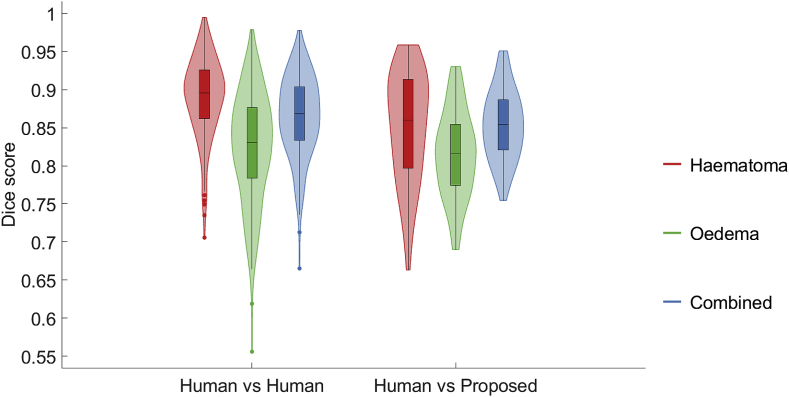
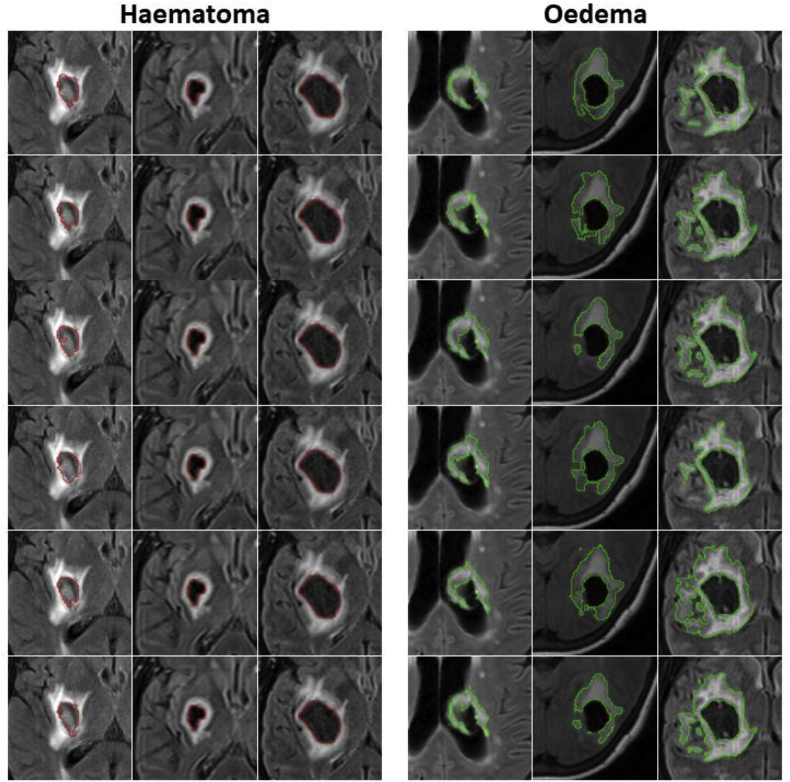
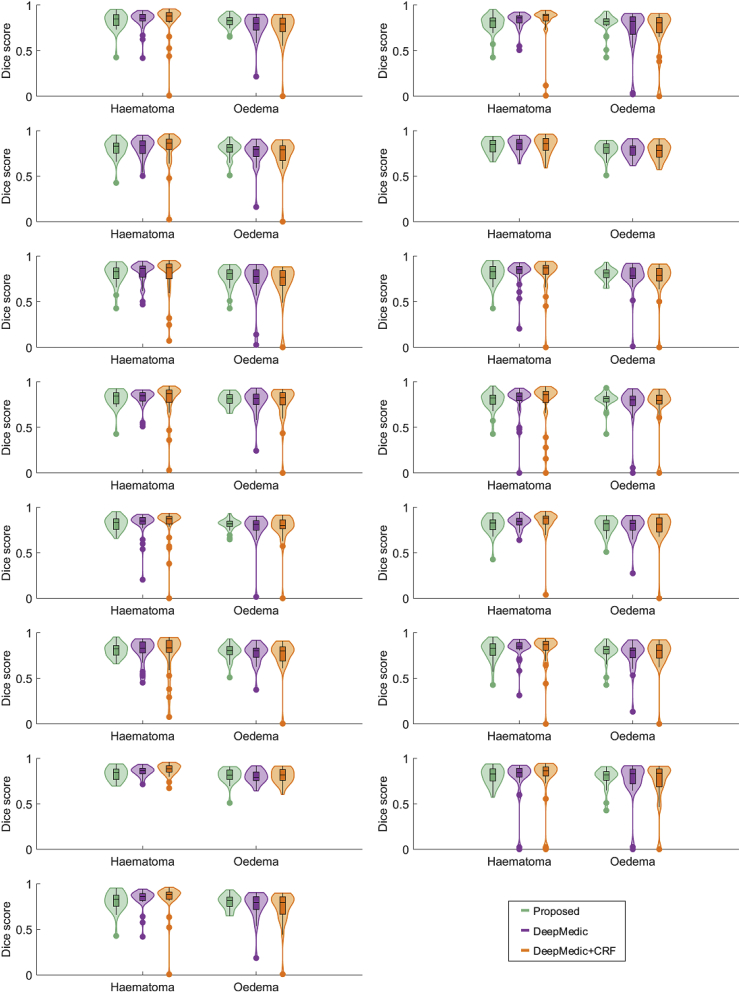
Results: Using Dice scores to measure segmentation overlaps between labellings yielded by the proposed algorithm and five different expert raters on 18 patients, we observe that our technique achieves overlap scores that are very similar to those obtained by pairwise expert rater comparison. A further comparison between the proposed method and a state-of-the-art Deep Learning segmentation on a separate set of 32 manually annotated subjects confirms the proposed method can achieve comparable results with very mild computational burden and in a completely training-free and unsupervised way.
Conclusion: Our technique can be a computationally light and effective way to automatically delineate haematoma and oedema extent directly from MR images. Thus, with increasing use of MR images clinically after intracerebral haemorrhage this technique has the potential to inform clinical practice in the future.
Keywords: Brain MRI; Image segmentation; Spontaneous intracerebral haemorrhage; Stroke.
Copyright © 2019. Published by Elsevier Ltd.
Figures


References
-
- Poon M.T.C., Fonville A.F., Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry. 2014;85:660–667. - PubMed
-
- van Asch C.J.J., Luitse M.J.A., Rinkel G.J.E., van der Tweel I., Algra A., Klijn C.J.M. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. - PubMed
-
- Appelboom G., Bruce S.S., Hickman Z.L., Zacharia B.E., Carpenter A.M., Vaughan K.A., Duren A., Hwang R.Y., Piazza M., Lee K., Claassen J., Mayer S., Badjatia N., Connolly E.S. Volume-dependent effect of perihaematomal oedema on outcome for spontaneous intracerebral haemorrhages. J. Neurol. Neurosurg. Psychiatry. 2013;84:488–493. - PubMed
-
- Lopresti M.A., Bruce S.S., Camacho E., Kunchala S., Dubois B.G., Bruce E., Appelboom G., Connolly E.S. Hematoma volume as the major determinant of outcomes after intracerebral hemorrhage. J. Neurol. Sci. 2014;345:3–7. - PubMed
-
- Yang J., Arima H., Wu G., Heeley E., Delcourt C., Zhou J., Chen G., Wang X., Zhang S., Yu S., Chalmers J., Anderson C.S. Prognostic significance of perihematomal edema in acute intracerebral hemorrhage: pooled analysis from the intensive blood pressure reduction in acute cerebral hemorrhage trial studies. Stroke. 2015;46:1009–1013. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
