

Predictive Model for High-Risk Coronary Artery Disease
- PMID: 30712364
- PMCID: PMC6368397
- DOI: 10.1161/CIRCIMAGING.118.007940
Predictive Model for High-Risk Coronary Artery Disease
Abstract
Background: Patients with high-risk coronary artery disease (CAD) may be difficult to identify.
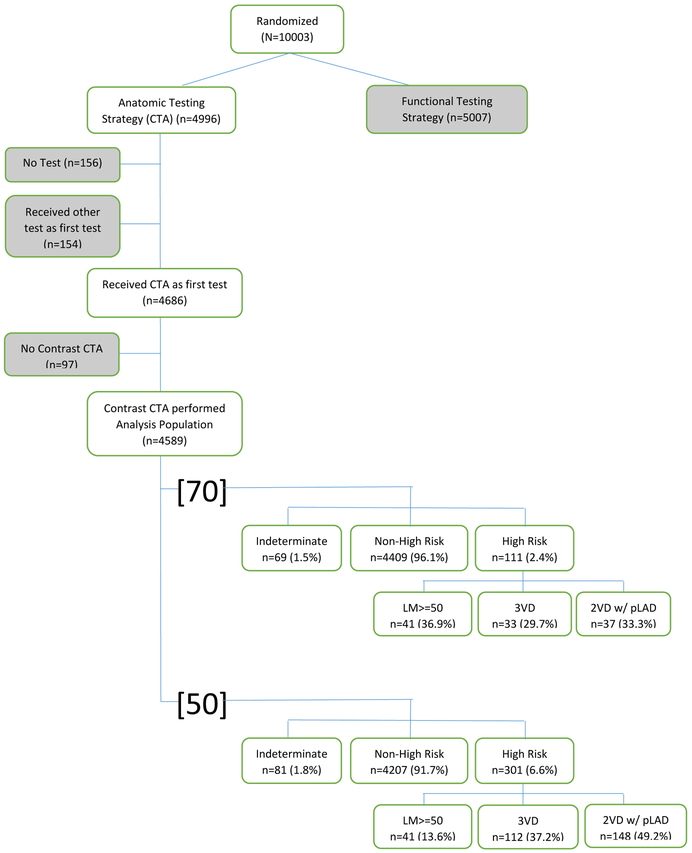
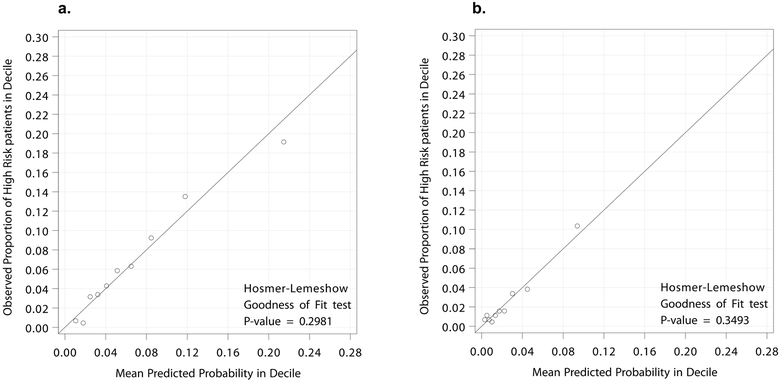
Methods: Using the PROMISE (Prospective Multicenter Imaging Study for Evaluation of Chest Pain) cohort randomized to coronary computed tomographic angiography (n=4589), 2 predictive models were developed for high-risk CAD, defined as left main stenosis (≥50% stenosis) or either (1) ≥50% stenosis [50] or (2) ≥70% stenosis [70] of 3 vessels or 2-vessel CAD involving the proximal left anterior descending artery. Pretest predictors were examined using stepwise logistic regression and assessed for discrimination and calibration.
Results: High-risk CAD was identified in 6.6% [50] and 2.4% [70] of patients. Models developed to predict high-risk CAD discriminated well: [50], bias-corrected C statistic=0.73 (95% CI, 0.71-0.76); [70], bias-corrected C statistic=0.73 (95% CI, 0.68-0.77). Variables predictive of CAD in both models included family history of premature CAD, age, male sex, lower glomerular filtration rate, diabetes mellitus, elevated systolic blood pressure, and angina. Additionally, smoking history was predictive of [50] CAD and sedentary lifestyle of [70] CAD. Both models characterized high-risk CAD better than the Pooled Cohort Equation (area under the curve=0.70 and 0.71 for [50] and [70], respectively) and Diamond-Forrester risk scores (area under the curve=0.68 and 0.71, respectively). Both [50] and [70] CAD was associated with more frequent invasive interventions and adverse events than non-high-risk CAD (all P<0.0001).
Conclusions: In contemporary practice, 2.4% to 6.6% of stable, symptomatic patients requiring noninvasive testing have high-risk CAD. A simple combination of pretest clinical variables improves prediction of high-risk CAD over traditional risk assessments.
Clinical trial registration: URL: https://www.clinicaltrials.gov . Unique identifier: NCT01174550.
Keywords: angiography; coronary artery disease; risk assessment.
Figures
Comment in
-
Clinical Risk Scores to Minimize Low Yield Coronary Artery Disease Testing.Circ Cardiovasc Imaging. 2019 Feb;12(2):e008626. doi: 10.1161/CIRCIMAGING.118.008626. Circ Cardiovasc Imaging. 2019. PMID: 30712365 Free PMC article. No abstract available.
References
-
- Emond Mock MB, Davis KB, Fisher LD, Holmes DR Jr, Chaitman BR, Kaiser GC, Alderman E, Killip T 3rd. Long-term survival of medically treated patients in the Coronary Artery Surgery Study (CASS) Registry. Circulation. 1994;90:2645–2657. - PubMed
-
- Leipsic J, Taylor CM, Grunau G, Heilbron BG, Mancini GB, Achenbach S, Al-Mallah M, Berman DS, Budoff MJ, Cademartiri F, Callister TQ, Chang HJ, Cheng VY, Chinnaiyan K, Chow BJ, Delago A, Hadamitzky M, Hausleiter J, Cury R, Feuchtner G, Kim YJ, Kaufmann PA, Lin FY, Maffei E, Raff G, Shaw LJ, Villines TC, Min JK. Cardiovascular risk among stable individuals suspected of having coronary artery disease with no modifiable risk factors: results from an international multicenter study of 5262 patients. Radiology. 2013;267:718–726. - PubMed
-
- Carrigan TP, Nair D, Schoenhagen P, Curtin RJ, Popovic ZB, Halliburton S, Kuzmiak S, White RD, Flamm SD, Desai MY. Prognostic utility of 64-slice computed tomography in patients with suspected but no documented coronary artery disease. Eur Heart J. 2009;30:362–371. - PubMed
-
- Caracciolo EA, Davis KB, Sopko G, Kaiser GC, Corley SD, Schaff H, Taylor HA, Chaitman BR. Comparison of surgical and medical group survival in patients with left main equivalent coronary artery disease. Long-term CASS experience. Circulation. 1995;91:2335–2344. - PubMed
-
- Takaro T, Hultgren HN, Lipton MJ, Detre KM. The VA cooperative randomized study of surgery for coronary arterial occlusive disease. II. Subgroup with significant left main lesions. Circulation. 1976;54(suppl III):107–117. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
