

Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): a cohort study
- PMID: 30712880
- PMCID: PMC6386638
- DOI: 10.1016/S0140-6736(18)31940-8
Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): a cohort study
Abstract
Background: Fetal structural anomalies, which are detected by ultrasonography, have a range of genetic causes, including chromosomal aneuploidy, copy number variations (CNVs; which are detectable by chromosomal microarrays), and pathogenic sequence variants in developmental genes. Testing for aneuploidy and CNVs is routine during the investigation of fetal structural anomalies, but there is little information on the clinical usefulness of genome-wide next-generation sequencing in the prenatal setting. We therefore aimed to evaluate the proportion of fetuses with structural abnormalities that had identifiable variants in genes associated with developmental disorders when assessed with whole-exome sequencing (WES).
Methods: In this prospective cohort study, two groups in Birmingham and London recruited patients from 34 fetal medicine units in England and Scotland. We used whole-exome sequencing (WES) to evaluate the presence of genetic variants in developmental disorder genes (diagnostic genetic variants) in a cohort of fetuses with structural anomalies and samples from their parents, after exclusion of aneuploidy and large CNVs. Women were eligible for inclusion if they were undergoing invasive testing for identified nuchal translucency or structural anomalies in their fetus, as detected by ultrasound after 11 weeks of gestation. The partners of these women also had to consent to participate. Sequencing results were interpreted with a targeted virtual gene panel for developmental disorders that comprised 1628 genes. Genetic results related to fetal structural anomaly phenotypes were then validated and reported postnatally. The primary endpoint, which was assessed in all fetuses, was the detection of diagnostic genetic variants considered to have caused the fetal developmental anomaly.
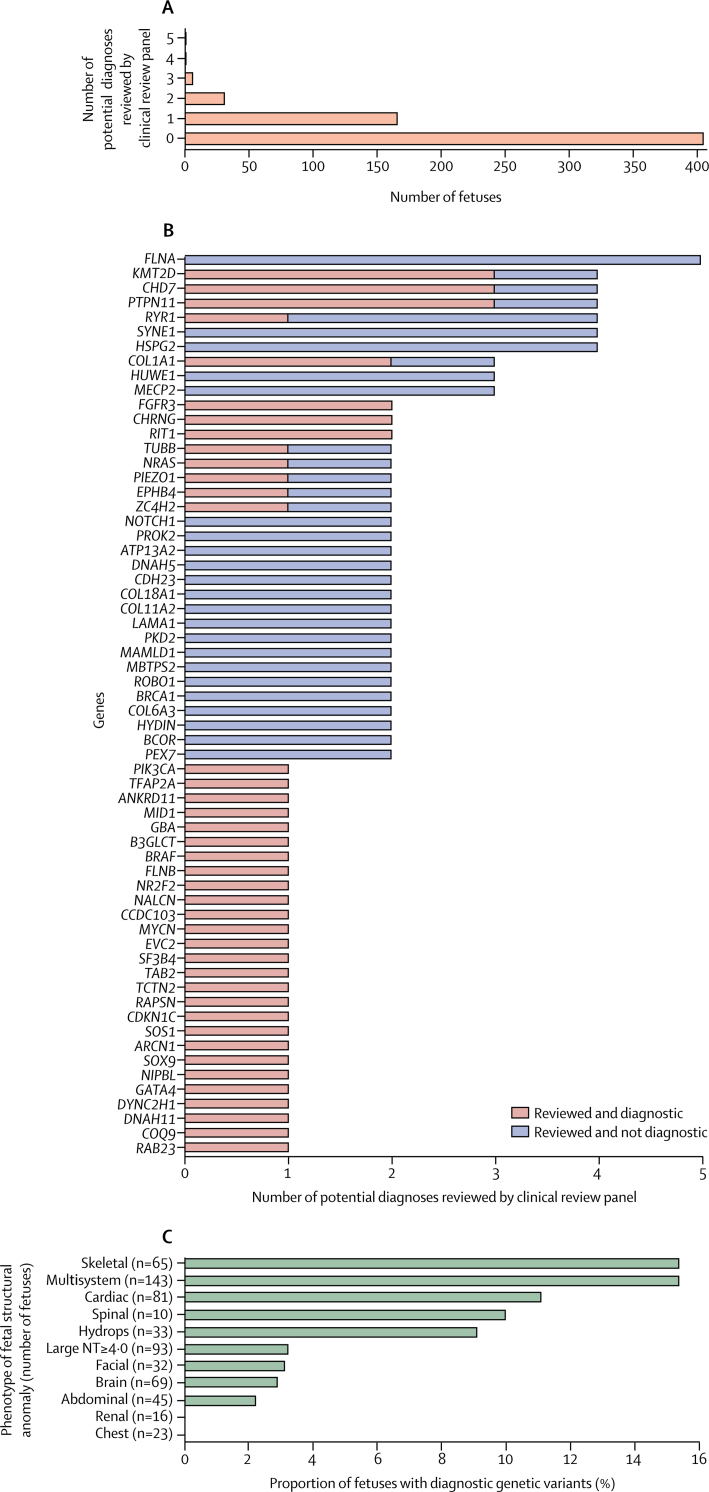
Findings: The cohort was recruited between Oct 22, 2014, and June 29, 2017, and clinical data were collected until March 31, 2018. After exclusion of fetuses with aneuploidy and CNVs, 610 fetuses with structural anomalies and 1202 matched parental samples (analysed as 596 fetus-parental trios, including two sets of twins, and 14 fetus-parent dyads) were analysed by WES. After bioinformatic filtering and prioritisation according to allele frequency and effect on protein and inheritance pattern, 321 genetic variants (representing 255 potential diagnoses) were selected as potentially pathogenic genetic variants (diagnostic genetic variants), and these variants were reviewed by a multidisciplinary clinical review panel. A diagnostic genetic variant was identified in 52 (8·5%; 95% CI 6·4-11·0) of 610 fetuses assessed and an additional 24 (3·9%) fetuses had a variant of uncertain significance that had potential clinical usefulness. Detection of diagnostic genetic variants enabled us to distinguish between syndromic and non-syndromic fetal anomalies (eg, congenital heart disease only vs a syndrome with congenital heart disease and learning disability). Diagnostic genetic variants were present in 22 (15·4%) of 143 fetuses with multisystem anomalies (ie, more than one fetal structural anomaly), nine (11·1%) of 81 fetuses with cardiac anomalies, and ten (15·4%) of 65 fetuses with skeletal anomalies; these phenotypes were most commonly associated with diagnostic variants. However, diagnostic genetic variants were least common in fetuses with isolated increased nuchal translucency (≥4·0 mm) in the first trimester (in three [3·2%] of 93 fetuses).
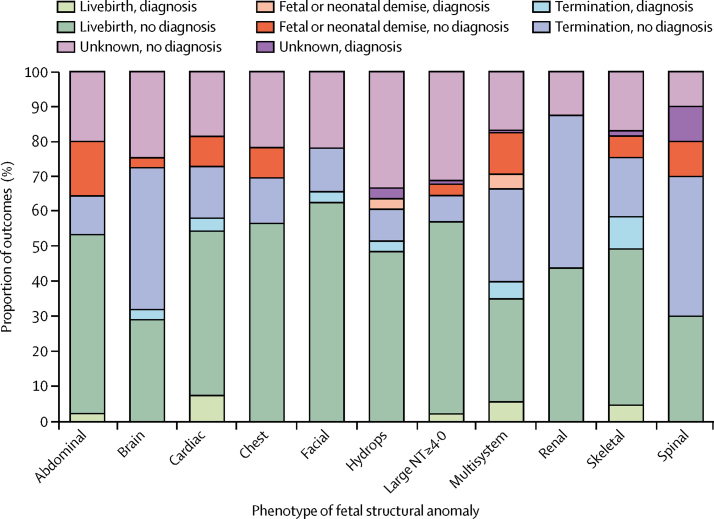
Interpretation: WES facilitates genetic diagnosis of fetal structural anomalies, which enables more accurate predictions of fetal prognosis and risk of recurrence in future pregnancies. However, the overall detection of diagnostic genetic variants in a prospectively ascertained cohort with a broad range of fetal structural anomalies is lower than that suggested by previous smaller-scale studies of fewer phenotypes. WES improved the identification of genetic disorders in fetuses with structural abnormalities; however, before clinical implementation, careful consideration should be given to case selection to maximise clinical usefulness.
Funding: UK Department of Health and Social Care and The Wellcome Trust.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Introduction of genomics into prenatal diagnostics.Lancet. 2019 Feb 23;393(10173):719-721. doi: 10.1016/S0140-6736(19)30193-X. Epub 2019 Jan 31. Lancet. 2019. PMID: 30712881 No abstract available.
-
Fetal medicine: past, present, and future.Lancet. 2019 Feb 23;393(10173):717. doi: 10.1016/S0140-6736(19)30404-0. Lancet. 2019. PMID: 30799000 No abstract available.
-
Is it feasible to select fetuses for prenatal WES based on the prenatal phenotype?Prenat Diagn. 2019 Oct;39(11):1039-1040. doi: 10.1002/pd.5522. Epub 2019 Sep 10. Prenat Diagn. 2019. PMID: 31506969 Free PMC article. No abstract available.
References
-
- Robson SC, Chitty LS, Morris S. Evaluation of array comparative genomic hybridisation in prenatal diagnosis of fetal anomalies: a multicentre cohort study with cost analysis and assessment of patient, health professional and commissioner preferences for array comparative genomic hybridisation. Effic Mech Eval. 2017;4:1–104. - PubMed
-
- Hillman SC, Pretlove S, Coomarasamy A. Additional information from array comparative genomic hybridization technology over conventional karyotyping in prenatal diagnosis: a systematic review and meta-analysis. Ultrasound Obstet Gynecol. 2011;37:6–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
