

Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials
- PMID: 30712900
- PMCID: PMC6429627
- DOI: 10.1016/S0140-6736(18)31942-1
Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials
Abstract
Background: Statin therapy has been shown to reduce major vascular events and vascular mortality in a wide range of individuals, but there is uncertainty about its efficacy and safety among older people. We undertook a meta-analysis of data from all large statin trials to compare the effects of statin therapy at different ages.
Methods: In this meta-analysis, randomised trials of statin therapy were eligible if they aimed to recruit at least 1000 participants with a scheduled treatment duration of at least 2 years. We analysed individual participant data from 22 trials (n=134 537) and detailed summary data from one trial (n=12 705) of statin therapy versus control, plus individual participant data from five trials of more intensive versus less intensive statin therapy (n=39 612). We subdivided participants into six age groups (55 years or younger, 56-60 years, 61-65 years, 66-70 years, 71-75 years, and older than 75 years). We estimated effects on major vascular events (ie, major coronary events, strokes, and coronary revascularisations), cause-specific mortality, and cancer incidence as the rate ratio (RR) per 1·0 mmol/L reduction in LDL cholesterol. We compared proportional risk reductions in different age subgroups by use of standard χ2 tests for heterogeneity when there were two groups, or trend when there were more than two groups.
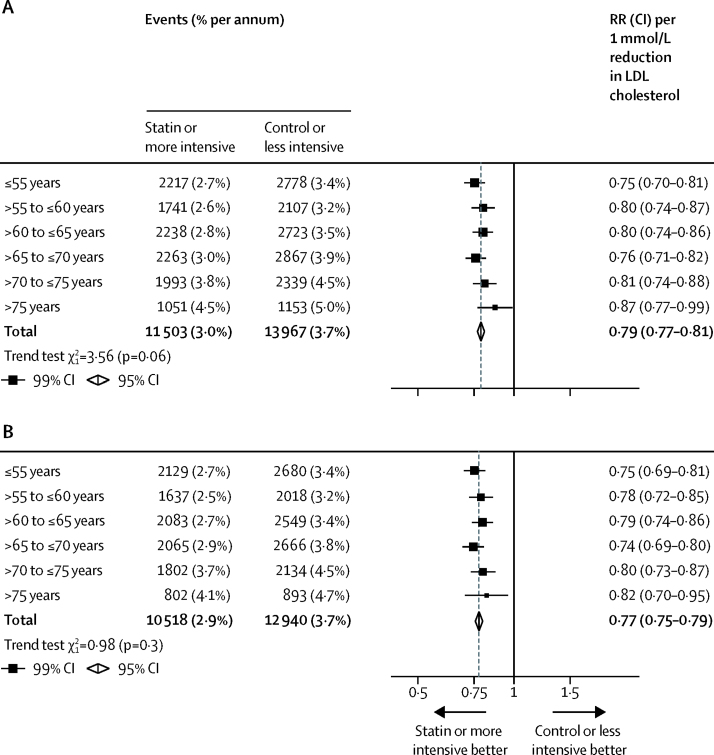
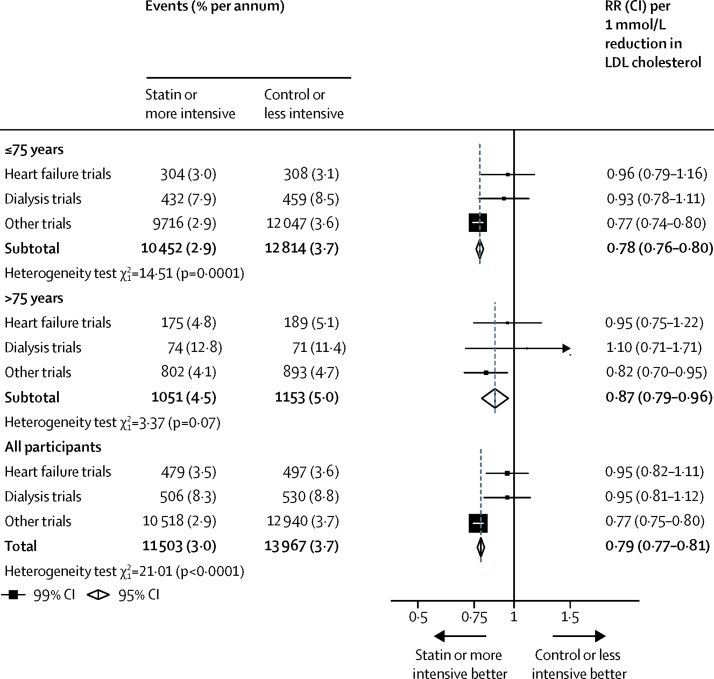
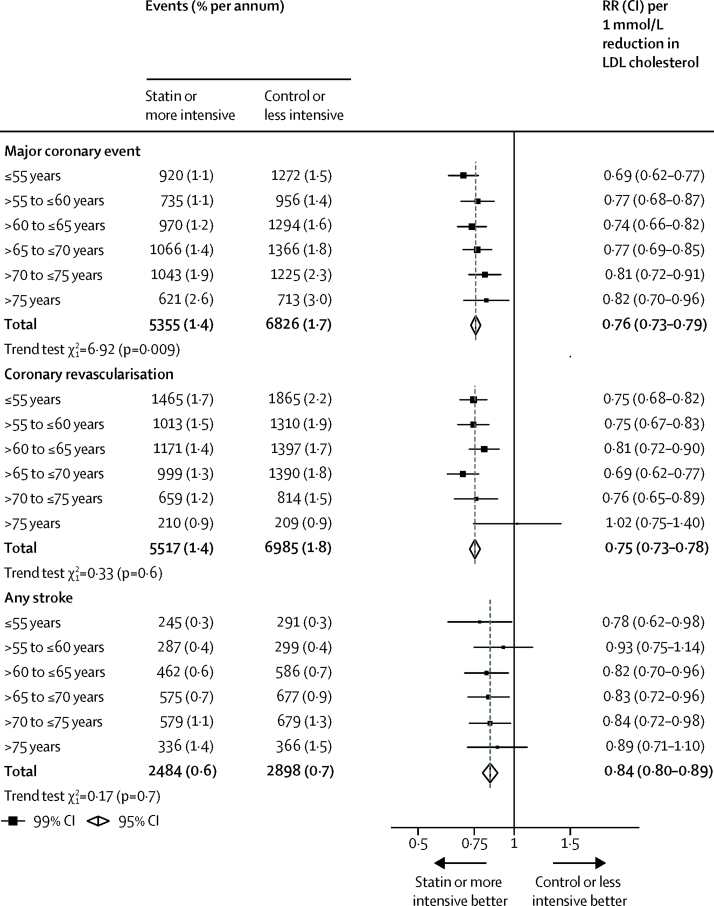
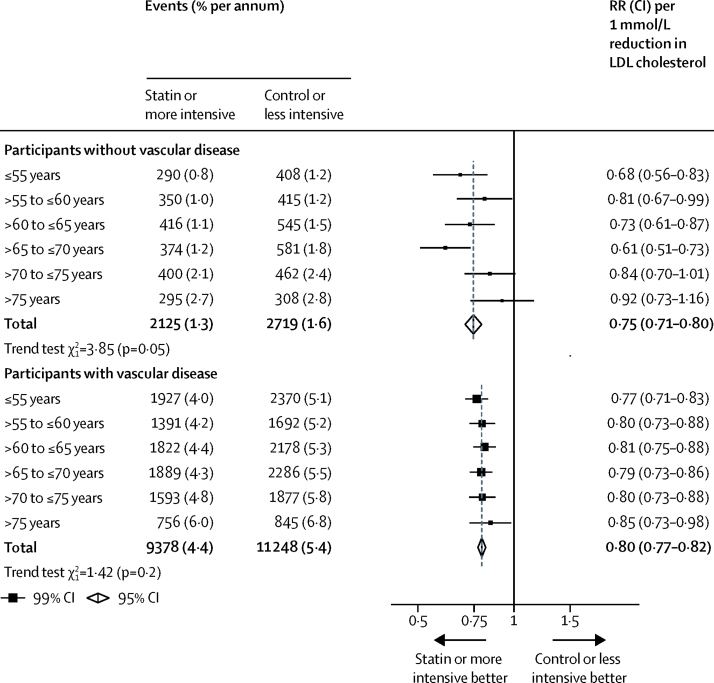
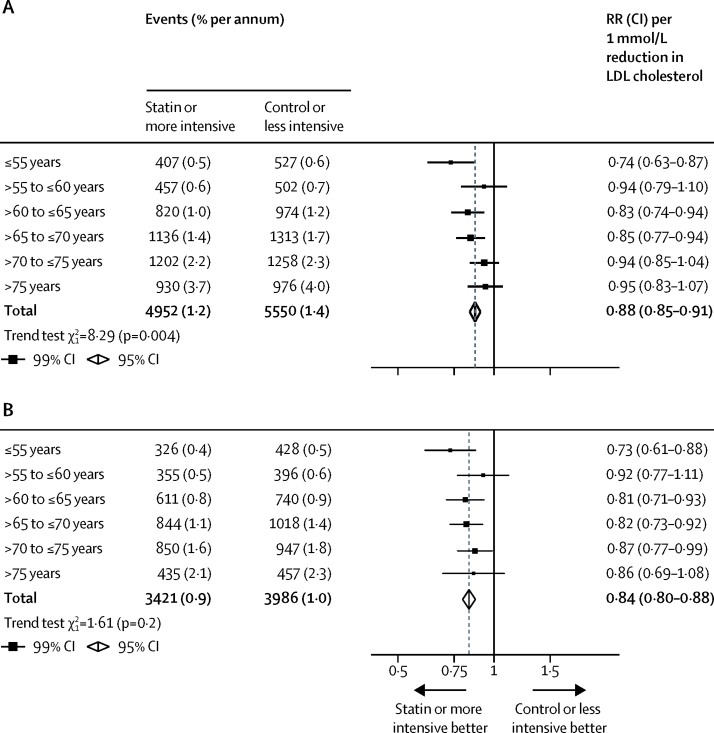
Findings: 14 483 (8%) of 186 854 participants in the 28 trials were older than 75 years at randomisation, and the median follow-up duration was 4·9 years. Overall, statin therapy or a more intensive statin regimen produced a 21% (RR 0·79, 95% CI 0·77-0·81) proportional reduction in major vascular events per 1·0 mmol/L reduction in LDL cholesterol. We observed a significant reduction in major vascular events in all age groups. Although proportional reductions in major vascular events diminished slightly with age, this trend was not statistically significant (ptrend=0·06). Overall, statin or more intensive therapy yielded a 24% (RR 0·76, 95% CI 0·73-0·79) proportional reduction in major coronary events per 1·0 mmol/L reduction in LDL cholesterol, and with increasing age, we observed a trend towards smaller proportional risk reductions in major coronary events (ptrend=0·009). We observed a 25% (RR 0·75, 95% CI 0·73-0·78) proportional reduction in the risk of coronary revascularisation procedures with statin therapy or a more intensive statin regimen per 1·0 mmol/L lower LDL cholesterol, which did not differ significantly across age groups (ptrend=0·6). Similarly, the proportional reductions in stroke of any type (RR 0·84, 95% CI 0·80-0·89) did not differ significantly across age groups (ptrend=0·7). After exclusion of four trials which enrolled only patients with heart failure or undergoing renal dialysis (among whom statin therapy has not been shown to be effective), the trend to smaller proportional risk reductions with increasing age persisted for major coronary events (ptrend=0·01), and remained non-significant for major vascular events (ptrend=0·3). The proportional reduction in major vascular events was similar, irrespective of age, among patients with pre-existing vascular disease (ptrend=0·2), but appeared smaller among older than among younger individuals not known to have vascular disease (ptrend=0·05). We found a 12% (RR 0·88, 95% CI 0·85-0·91) proportional reduction in vascular mortality per 1·0 mmol/L reduction in LDL cholesterol, with a trend towards smaller proportional reductions with older age (ptrend=0·004), but this trend did not persist after exclusion of the heart failure or dialysis trials (ptrend=0·2). Statin therapy had no effect at any age on non-vascular mortality, cancer death, or cancer incidence.
Interpretation: Statin therapy produces significant reductions in major vascular events irrespective of age, but there is less direct evidence of benefit among patients older than 75 years who do not already have evidence of occlusive vascular disease. This limitation is now being addressed by further trials.
Funding: Australian National Health and Medical Research Council, National Institute for Health Research Oxford Biomedical Research Centre, UK Medical Research Council, and British Heart Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Never too old for statin treatment?Lancet. 2019 Feb 2;393(10170):379-380. doi: 10.1016/S0140-6736(18)32263-3. Lancet. 2019. PMID: 30712888 No abstract available.
-
Absolute effects of statins in the elderly.BMJ Evid Based Med. 2019 Oct;24(5):200-202. doi: 10.1136/bmjebm-2019-111189. Epub 2019 May 15. BMJ Evid Based Med. 2019. PMID: 31092405 No abstract available.
-
Pooled RCTs: Lowering LDL-C levels using statins reduces major vascular events in all age groups.Ann Intern Med. 2019 Jun 18;170(12):JC65. doi: 10.7326/ACPJ201906180-065. Ann Intern Med. 2019. PMID: 31207618 No abstract available.
-
PURL: How old is too old for statins?J Fam Pract. 2020 Jun;69(5):257-259. J Fam Pract. 2020. PMID: 32555755 Free PMC article.
References
-
- Cholesterol Treatment Trialists (CTT) Collaboration Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174 000 participants in 27 randomised trials. Lancet. 2015;385:1397–1405. - PubMed
-
- Koopman C, Vaartjes I, Heintjes EM. Persisting gender differences and attenuating age differences in cardiovascular drug use for prevention and treatment of coronary heart disease, 1998–2010. Eur Heart J. 2013;34:3198–3205. - PubMed
-
- Salami JA, Warraich H, Valero-Elizondo J. National trends in statin use and expenditures in the US adult population from 2002 to 2013: insights from the Medical Expenditure Panel Survey. JAMA Cardiol. 2017;2:56–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
