

Impact of Immune and Stromal Infiltration on Outcomes Following Bladder-Sparing Trimodality Therapy for Muscle-Invasive Bladder Cancer
- PMID: 30712971
- PMCID: PMC6571058
- DOI: 10.1016/j.eururo.2019.01.011
Impact of Immune and Stromal Infiltration on Outcomes Following Bladder-Sparing Trimodality Therapy for Muscle-Invasive Bladder Cancer
Abstract
Background: Bladder-sparing trimodality therapy (TMT) is an alternative to radical cystectomy (RC) for muscle-invasive bladder cancer (MIBC), and biomarkers to inform therapy selection are needed.
Objective: To evaluate the prognostic value of immune and stromal signatures in MIBC treated with TMT.
Design, setting, and participants: We used a clinical-grade platform to perform transcriptome-wide gene expression profiling of primary tumors from 136 MIBC patients treated with TMT at a single institution. We observed 60 overall survival events at 5yr, and median follow-up time for patients without an event was 5.0yr (interquartile range 3.1, 5.0). Expression data from another cohort of 223 MIBC patients treated with neoadjuvant chemotherapy (NAC) and RC were also analyzed.
Outcome measurements and statistical analysis: Molecular subtype, immune, and stromal signatures were evaluated for associations with disease-specific survival (DSS) and overall survival (OS) in TMT patients, and in patients treated with NAC and RC.
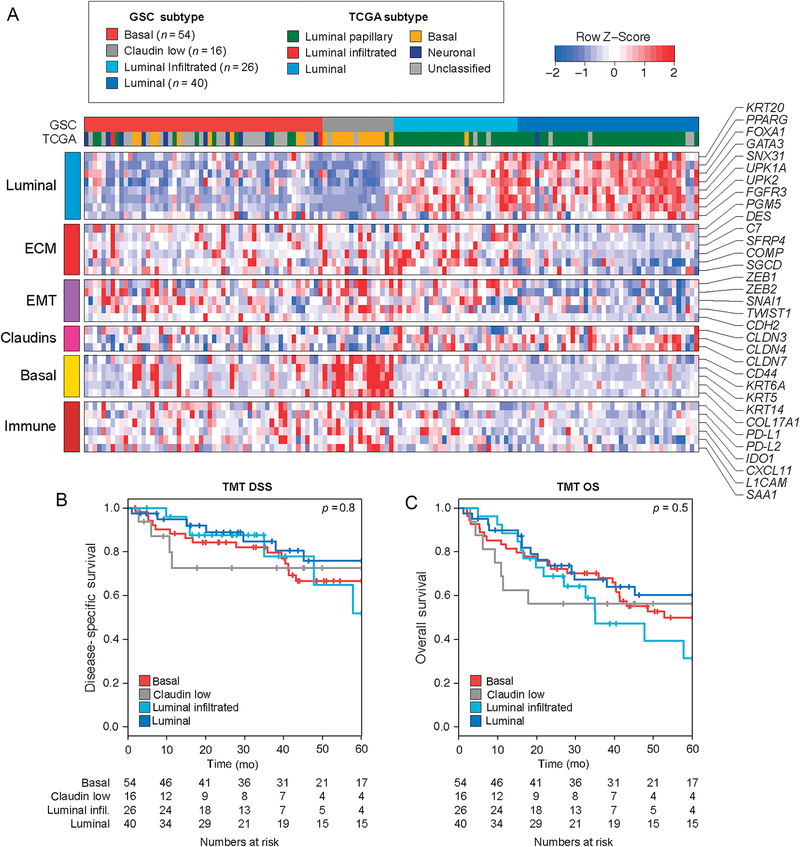
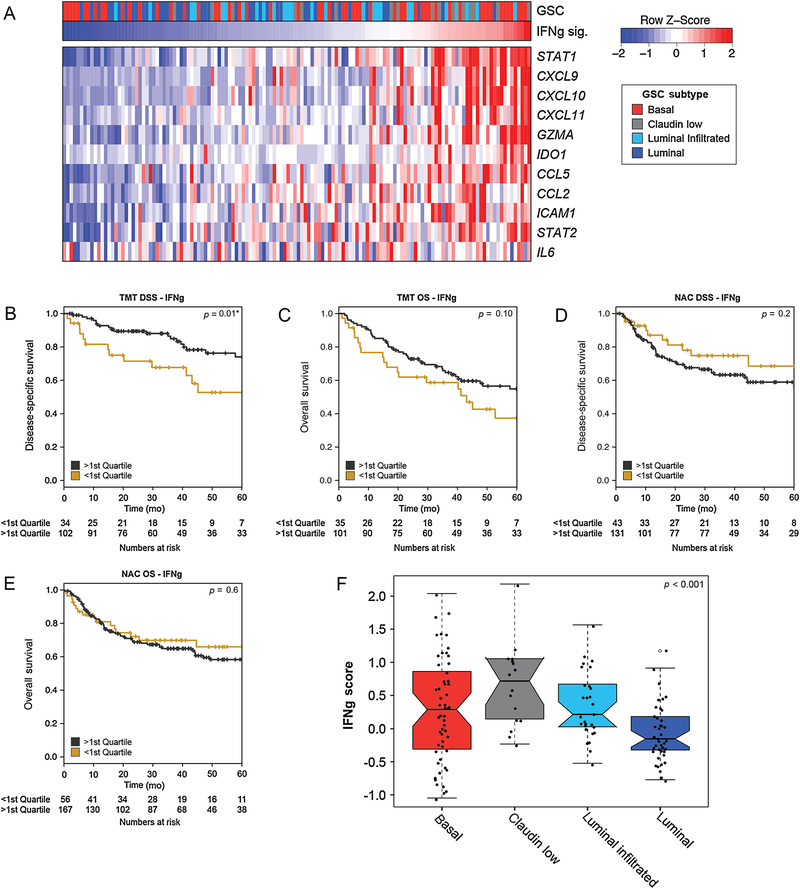
Results and limitations: Gene expression profiling of TMT cases identified luminal (N=40), luminal-infiltrated (N=26), basal (N=54), and claudin-low (N=16) subtypes. Signatures of T-cell activation and interferon gamma signaling were associated with improved DSS in the TMT cohort (hazard ratio 0.30 [0.14-0.65], p=0.002 for T cells), but not in the NAC and RC cohort. Conversely, a stromal signature was associated with worse DSS in the NAC and RC cohort (p=0.006), but not in the TMT cohort. This study is limited by its retrospective nature.
Conclusions: Higher immune infiltration in MIBC is associated with improved DSS after TMT, whereas higher stromal infiltration is associated with shorter DSS after NAC and RC. Additional studies should be conducted to determine whether gene expression profiling can predict treatment response.
Patient summary: We used gene expression profiling to study the association between tumor microenvironment and outcomes following bladder preservation therapy for invasive bladder cancer. We found that outcomes varied with immune and stromal signatures within the tumor. We conclude that gene expression profiling has potential to guide treatment decisions in bladder cancer.
Keywords: Biomarker; Bladder cancer; Bladder preservation; Bladder-sparing; Chemoradiation; Gene expression profiling; Immune; Muscle-invasive bladder cancer; Radiation; Stromal; Trimodality therapy.
Copyright © 2019 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures


Comment in
-
Predictive Biomarkers for Muscle-invasive Bladder Cancer: The Search for the Holy Grail Continues.Eur Urol. 2019 Jul;76(1):69-70. doi: 10.1016/j.eururo.2019.01.040. Epub 2019 Feb 4. Eur Urol. 2019. PMID: 30732925 No abstract available.
-
Re: Impact of Immune and Stromal Infiltration on Outcomes Following Bladder-sparing Trimodality Therapy for Muscle-invasive Bladder Cancer.Eur Urol. 2019 Jun;75(6):1034-1035. doi: 10.1016/j.eururo.2019.02.022. Epub 2019 Mar 2. Eur Urol. 2019. PMID: 30833138 No abstract available.
-
Reply from Authors re: Ananya Choudhury, Peter J. Hoskin. Predictive Biomarkers for Muscle-invasive Bladder Cancer: The Search for the Holy Grail Continues. Eur Urol 2019;76:69-70: Towards Biomarker-Informed Management of Muscle-Invasive Bladder Cancer.Eur Urol. 2019 Jul;76(1):71-72. doi: 10.1016/j.eururo.2019.03.009. Epub 2019 Mar 23. Eur Urol. 2019. PMID: 30910345 No abstract available.
-
Molecular subtyping, tumor infiltration, and trimodal therapy for muscle-invasive bladder cancer: more questions than answers.Transl Androl Urol. 2019 Jul;8(Suppl 3):S325-S328. doi: 10.21037/tau.2019.05.12. Transl Androl Urol. 2019. PMID: 31392159 Free PMC article. No abstract available.
-
How to guide the selection of patients for trimodality therapy: the case for tumor immune and stromal signature.Transl Androl Urol. 2019 Jul;8(Suppl 3):S329-S331. doi: 10.21037/tau.2019.05.10. Transl Androl Urol. 2019. PMID: 31392160 Free PMC article. No abstract available.
References
-
- National Comprehensive Cancer Network. Bladder cancer—version 3. 2018. https://www.nccn.org/professionals/physician_gls/PDF/bladder.pdf
-
- Gakis G, Efstathiou J, Lerner SP, et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Radical cystectomy and bladder preservation for muscle-invasive urothelial carcinoma of the bladder. Eur Urol 2013;63:45–57. - PubMed
-
- Huddart RA, Hall E, Lewis R, Birtle A, SPARE Trial Management Group. Life and death of spare (selective bladder preservation against radical excision): reflections on why the spare trial closed. BJU Int 2010;106:753–5. - PubMed
-
- Mak RH, Hunt D, Shipley WU, et al. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: a pooled analysis of Radiation Therapy Oncology Group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J Clin Oncol 2014;32:3801–9. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
