

Sex hormones and stroke: Beyond estrogens
- PMID: 30713101
- PMCID: PMC6527470
- DOI: 10.1016/j.yhbeh.2018.10.010
Sex hormones and stroke: Beyond estrogens
Abstract
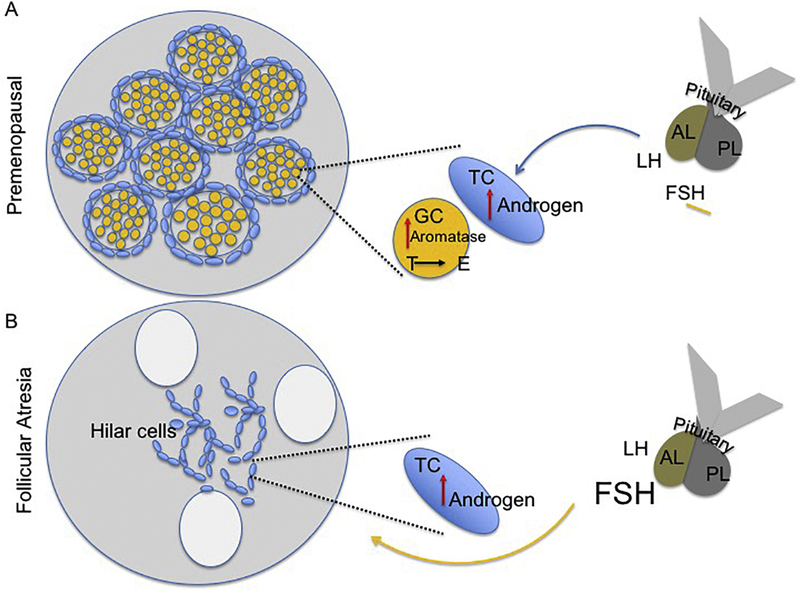
Stroke risk and poor stroke outcomes in postmenopausal women have usually beeen attributed to decreased levels of estrogen. However, two lines of evidence suggest that this hormone may not be solely responsible for elevated stroke risk in this population. First, the increased risk for CVD and stroke occurs much earlier than menopause at a time when estrogen levels are not yet reduced. Second, estrogen therapy has not successfully reduced stroke risk in all studies. Other sex hormones may therefore also contribute to stroke risk. Prior to menopause, levels of the gonadotrophin Follicle Stimulating Hormone (FSH) are elevated while levels of the gonadal peptide inhibin are lowered, indicating an overall decrease in ovarian reserve. Similarly, reduced estrogen levels at menopause significantly increase the ratio of androgens to estrogens. In view of the evidence that androgens may be unfavorable for CVD and stroke, this elevated ratio of testosterone to estrogen may also contribute to the postmenopause-associated stroke risk. This review synthesizes evidence from different clinical populations including natural menopause, surgical menopause, women on chemotherapy, and preclinical stroke models to dissect the role of ovarian hormones and stroke risk and outcomes.
Keywords: FSH; Ischemic stroke; Menopause; Testosterone.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
References
-
- Towfighi A, et al. , A midlife stroke surge among women in the United States. Neurology, 2007. 69(20): p. 1898–904. - PubMed
-
- Sohrabji F, Chapter 9 - Cerebrovascular Stroke: Sex Differences and the Impact of Estrogens A2 - Duncan, Kelli A, in Estrogen Effects on Traumatic Brain Injury. 2015, Academic Press: San Diego: p. 125–141.
-
- Lloyd-Jones D, et al. , Heart disease and stroke statistics−−2010 update: a report from the American Heart Association. Circulation, 2010. 121(7): p. e46–e215. - PubMed
-
- Kapral MK, et al. , Sex differences in stroke care and outcomes: results from the Registry of the Canadian Stroke Network. Stroke, 2005. 36(4): p. 809–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
