

Evaluation of Changes in Functional Status in the Year After Aortic Valve Replacement
- PMID: 30715097
- PMCID: PMC6439710
- DOI: 10.1001/jamainternmed.2018.6738
Evaluation of Changes in Functional Status in the Year After Aortic Valve Replacement
Abstract
Importance: Functional status is a patient-centered outcome that is important for a meaningful gain in health-related quality of life after aortic valve replacement.
Objective: To determine functional status trajectories in the year after transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR).
Design, setting, and participants: A prospective cohort study with a 12-month follow-up was conducted at a single academic center in 246 patients undergoing TAVR or SAVR for severe aortic stenosis. The study was conducted between February 1, 2014, and June 30, 2017; data analysis was performed from December 27, 2017, to May 7, 2018.
Exposures: Preoperative comprehensive geriatric assessment was performed and a deficit-accumulation frailty index (CGA-FI) (range, 0-1; higher values indicate greater frailty) was calculated.
Main outcomes and measures: Telephone interviews were conducted to assess self-reported ability to perform 22 activities and physical tasks at 1, 3, 6, 9, and 12 months after the procedure.
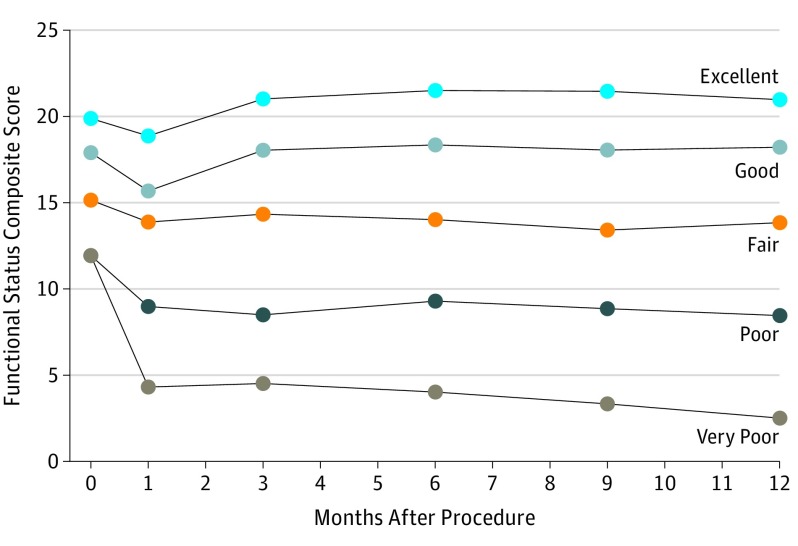
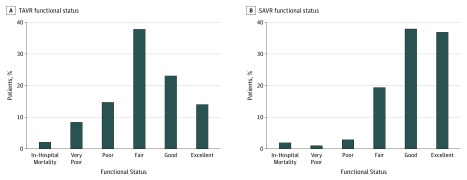
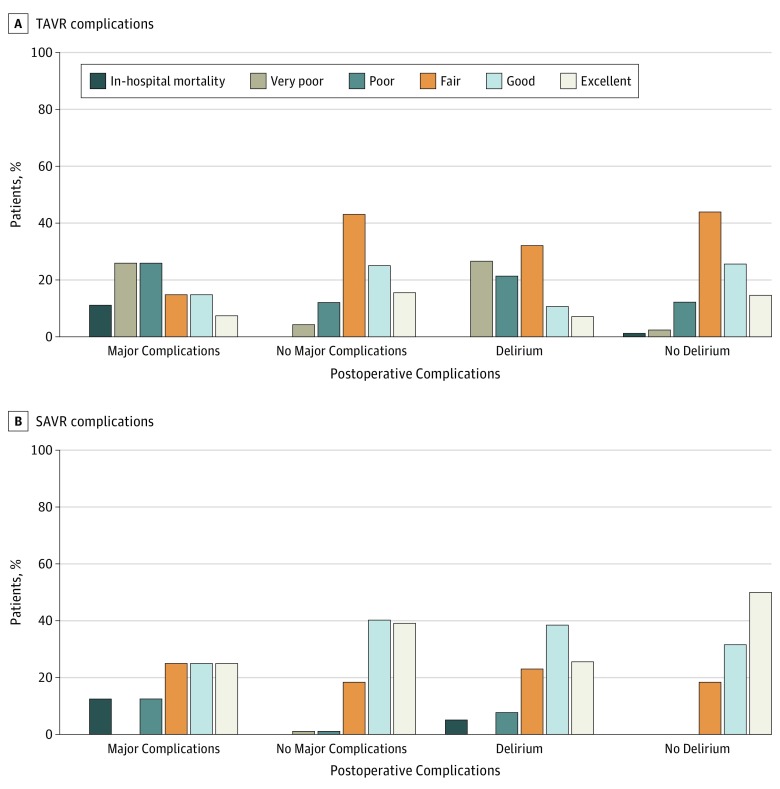
Results: Of the 246 patients included in the study, 143 underwent TAVR (74 [51.7%] women; mean [SD] age, 84.2 [5.9] years), and 103 underwent SAVR (46 [44.7%] women; age, 78.1 [5.3] years). Five trajectories were identified based on functional status at baseline and during the follow-up: from excellent at baseline to improvement at follow-up (excellent baseline-improvement), good (high baseline-full recovery), fair (moderate baseline-minimal decline), poor (low baseline-moderate decline), and very poor (low baseline-large decline). After TAVR, the most common trajectory was fair (54 [37.8%]), followed by good (33 [23.1%]), poor (21 [14.7%]), excellent (20 [14.0%]), and very poor (12 [8.4%]) trajectories. After SAVR, the most common trajectory was good (39 [37.9%]), followed by excellent (38 [36.9%]), fair (20 [19.4%]), poor (3 [2.9%]), and very poor (1 [1.0%]) trajectories. Preoperative frailty level was associated with lower probability of functional improvement and greater probability of functional decline. After TAVR, patients with CGA-FI level of 0.20 or lower had excellent (3 [50.0%]) or good (3 [50.0%]) trajectories, whereas most patients with CGA-FI level of 0.51 or higher had poor (10 [45.5%]) or very poor (5 [22.7%]) trajectories. After SAVR, most patients with CGA-FI level of 0.20 or lower had excellent (24 [58.5%]) or good (15 [36.6%]) trajectories compared with a fair trajectory (5 [71.4%]) in those with CGA-FI levels of 0.41 to 0.50. Postoperative delirium and major complications were associated with functional decline after TAVR (delirium present vs absent: 14 [50.0%] vs 11 [13.4%]; complications present vs absent: 14 [51.9%] vs 19 [16.4%]) or lack of improvement after SAVR (delirium present vs absent: 27 [69.2%] vs 31 [81.6%]; complications present vs absent: 10 [62.5%] vs 69 [79.3%]).
Conclusions and relevance: The findings suggest that functional decline or lack of improvement is common in older adults with severe frailty undergoing TAVR or SAVR. Although this nonrandomized study does not allow comparison of the effectiveness between TAVR and SAVR, anticipated functional trajectories may inform patient-centered decision making and perioperative care to optimize functional outcomes.
Conflict of interest statement
Figures
Comment in
-
Invasive Procedures to Improve Function in Frail Older Adults: Do Outcomes Justify the Intervention?JAMA Intern Med. 2019 Mar 1;179(3):391-393. doi: 10.1001/jamainternmed.2018.6708. JAMA Intern Med. 2019. PMID: 30715086 No abstract available.
Similar articles
-
A Practical Two-Stage Frailty Assessment for Older Adults Undergoing Aortic Valve Replacement.J Am Geriatr Soc. 2019 Oct;67(10):2031-2037. doi: 10.1111/jgs.16036. Epub 2019 Jun 18. J Am Geriatr Soc. 2019. PMID: 31211413 Free PMC article.
-
Frailty Phenotype and Deficit Accumulation Frailty Index in Predicting Recovery After Transcatheter and Surgical Aortic Valve Replacement.J Gerontol A Biol Sci Med Sci. 2019 Jul 12;74(8):1249-1256. doi: 10.1093/gerona/gly196. J Gerontol A Biol Sci Med Sci. 2019. PMID: 30165422 Free PMC article.
-
Health Status Benefits of Transcatheter vs Surgical Aortic Valve Replacement in Patients With Severe Aortic Stenosis at Intermediate Surgical Risk: Results From the PARTNER 2 Randomized Clinical Trial.JAMA Cardiol. 2017 Aug 1;2(8):837-845. doi: 10.1001/jamacardio.2017.2039. JAMA Cardiol. 2017. PMID: 28658491 Free PMC article. Clinical Trial.
-
Transcatheter vs. surgical aortic valve replacement and medical treatment : Systematic review and meta-analysis of randomized and non-randomized trials.Herz. 2018 Jun;43(4):325-337. doi: 10.1007/s00059-017-4562-5. Epub 2017 Apr 27. Herz. 2018. PMID: 28451702 English.
-
Transcatheter aortic valve replacement versus surgical aortic valve replacement in low-surgical-risk patients: An updated meta-analysis.Catheter Cardiovasc Interv. 2020 Jul;96(1):169-178. doi: 10.1002/ccd.28520. Epub 2019 Oct 21. Catheter Cardiovasc Interv. 2020. PMID: 31631514
Cited by
-
Validation of the Korean Frailty Index in community-dwelling older adults in a nationwide Korean Frailty and Aging Cohort study.Korean J Intern Med. 2021 Mar;36(2):456-466. doi: 10.3904/kjim.2019.172. Epub 2020 Apr 17. Korean J Intern Med. 2021. PMID: 32299182 Free PMC article.
-
Validity of the Clinical Frailty Scale in Korean older patients at a geriatric clinic.Korean J Intern Med. 2021 Sep;36(5):1242-1250. doi: 10.3904/kjim.2020.652. Epub 2020 Dec 30. Korean J Intern Med. 2021. PMID: 34503320 Free PMC article.
-
Association between clinical frailty, illness severity and post-discharge survival: a prospective cohort study of older medical inpatients in Norway.Eur Geriatr Med. 2022 Apr;13(2):453-461. doi: 10.1007/s41999-021-00555-8. Epub 2021 Aug 21. Eur Geriatr Med. 2022. PMID: 34417977 Free PMC article.
-
Long-Term Outcome of Elderly Patients with Severe Aortic Stenosis Undergoing a Tailored Interventional Treatment Using Frailty-Based Management: Beyond the Five-Year Horizon.J Pers Med. 2024 Dec 21;14(12):1164. doi: 10.3390/jpm14121164. J Pers Med. 2024. PMID: 39728076 Free PMC article.
-
From research to bedside: Incorporation of a CGA-based frailty index among multiple comanagement services.J Am Geriatr Soc. 2022 Jan;70(1):90-98. doi: 10.1111/jgs.17446. Epub 2021 Sep 13. J Am Geriatr Soc. 2022. PMID: 34519037 Free PMC article.
References
-
- Arnold SV, Reynolds MR, Lei Y, et al. ; PARTNER Investigators . Predictors of poor outcomes after transcatheter aortic valve replacement: results from the PARTNER (Placement of Aortic Transcatheter Valve) trial. Circulation. 2014;129(25):2682-2690. doi:10.1161/CIRCULATIONAHA.113.007477 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
