

Early Subthreshold Aerobic Exercise for Sport-Related Concussion: A Randomized Clinical Trial
- PMID: 30715132
- PMCID: PMC6450274
- DOI: 10.1001/jamapediatrics.2018.4397
Early Subthreshold Aerobic Exercise for Sport-Related Concussion: A Randomized Clinical Trial
Abstract
Importance: Sport-related concussion (SRC) is a significant public health problem without an effective treatment.
Objective: To assess the effectiveness of subsymptom threshold aerobic exercise vs a placebo-like stretching program prescribed to adolescents in the acute phase of recovery from SRC.
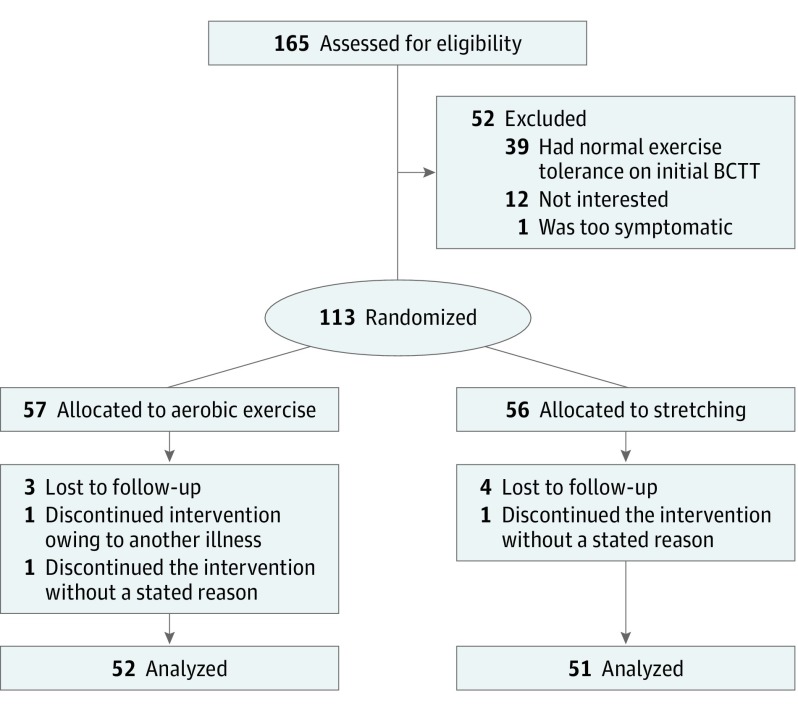
Design, setting, and participants: This multicenter prospective randomized clinical trial was conducted at university concussion centers. Male and female adolescent athletes (age 13-18 years) presenting within 10 days of SRC were randomly assigned to aerobic exercise or a placebo-like stretching regimen.
Interventions: After systematic determination of treadmill exercise tolerance on the first visit, participants were randomly assigned to a progressive subsymptom threshold aerobic exercise or a progressive placebo-like stretching program (that would not substantially elevate heart rate). Both forms of exercise were performed approximately 20 minutes per day, and participants reported daily symptoms and compliance with exercise prescription via a website.
Main outcomes and measures: Days from injury to recovery; recovery was defined as being asymptomatic, having recovery confirmed through an assessment by a physician blinded to treatment group, and returning to normal exercise tolerance on treadmill testing. Participants were also classified as having normal (<30 days) or delayed (≥30 days) recovery.
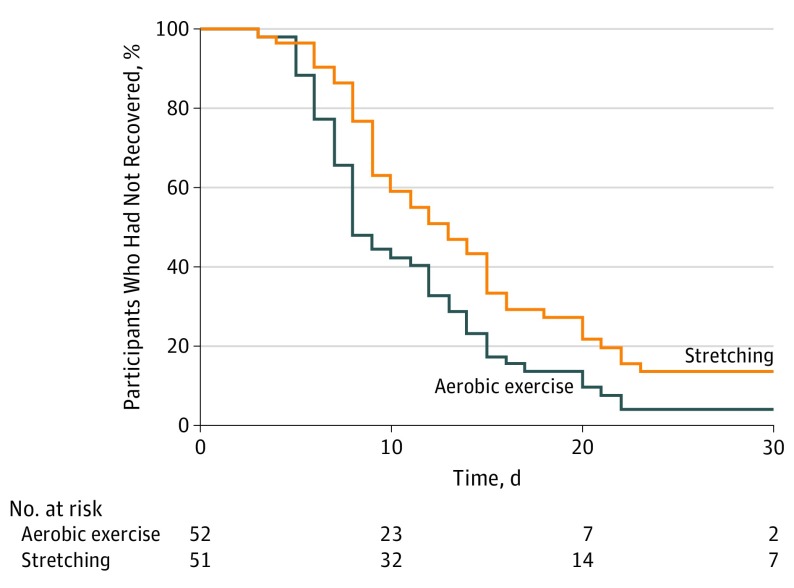
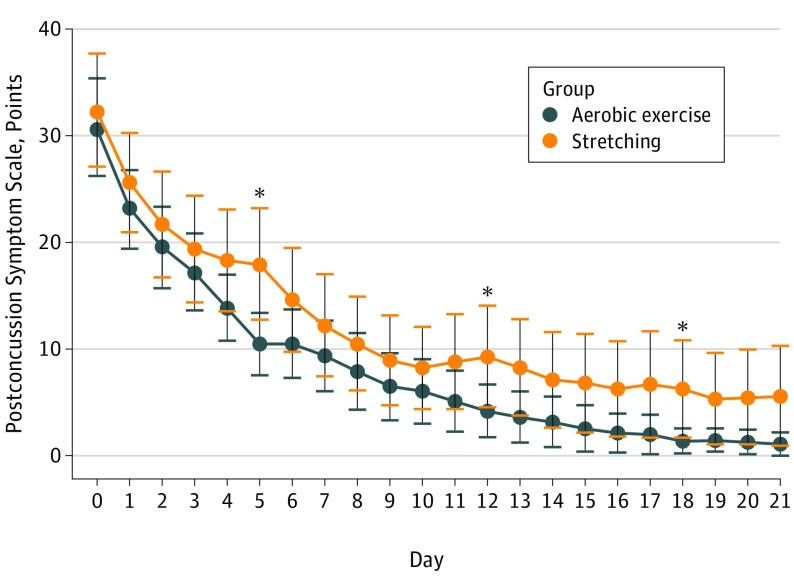
Results: A total of 103 participants were included (aerobic exercise: n = 52; 24 female [46%]; stretching, n = 51; 24 female [47%]). Participants in the aerobic exercise group were seen a mean (SD) of 4.9 (2.2) days after the SRC, and those in the stretching group were seen a mean (SD) of 4.8 (2.4) days after the SRC. There were no differences in age, sex, previous concussions, time from injury, initial symptom severity score, or initial exercise treadmill test and physical examination results. Aerobic exercise participants recovered in a median of 13 (interquartile range [IQR], 10-18.5) days, whereas stretching participants recovered in 17 (IQR, 13-23) days (P = .009 by Mann-Whitney test). There was a nonsignificant lower incidence of delayed recovery in the aerobic exercise group (2 participants [4%] in the aerobic group vs 7 [14%] in the placebo group; P = .08).
Conclusions and relevance: This is, to our knowledge, the first RCT to show that individualized subsymptom threshold aerobic exercise treatment prescribed to adolescents with concussion symptoms during the first week after SRC speeds recovery and may reduce the incidence of delayed recovery.
Trial registration: ClinicalTrials.gov identifier: NCT02710123.
Conflict of interest statement
Figures
Comment in
-
Exercise and Recovery Time for Youth With Concussions.JAMA Pediatr. 2019 Apr 1;173(4):315-316. doi: 10.1001/jamapediatrics.2018.5281. JAMA Pediatr. 2019. PMID: 30715089 No abstract available.
