

Lifetime risk and multimorbidity of non-communicable diseases and disease-free life expectancy in the general population: A population-based cohort study
- PMID: 30716101
- PMCID: PMC6361416
- DOI: 10.1371/journal.pmed.1002741
Lifetime risk and multimorbidity of non-communicable diseases and disease-free life expectancy in the general population: A population-based cohort study
Abstract
Background: Non-communicable diseases (NCDs) are leading causes of premature disability and death worldwide. However, the lifetime risk of developing any NCD is unknown, as are the effects of shared common risk factors on this risk.
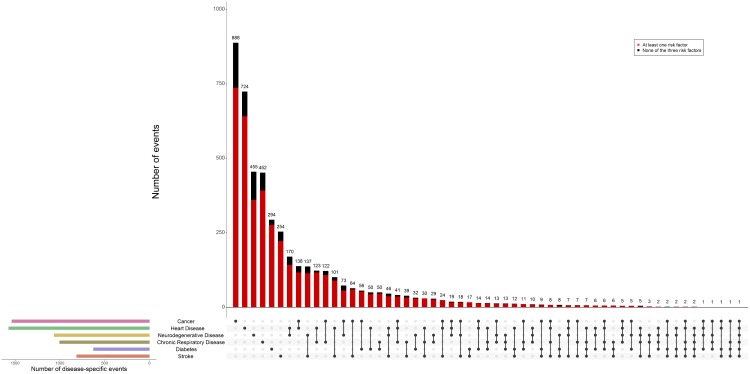
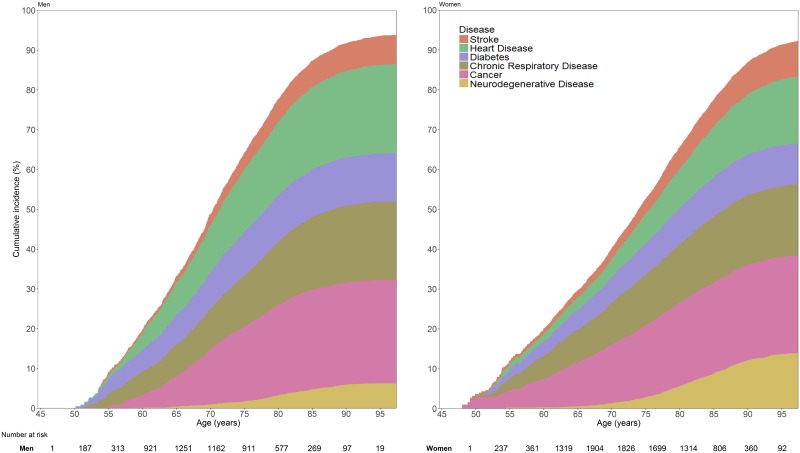
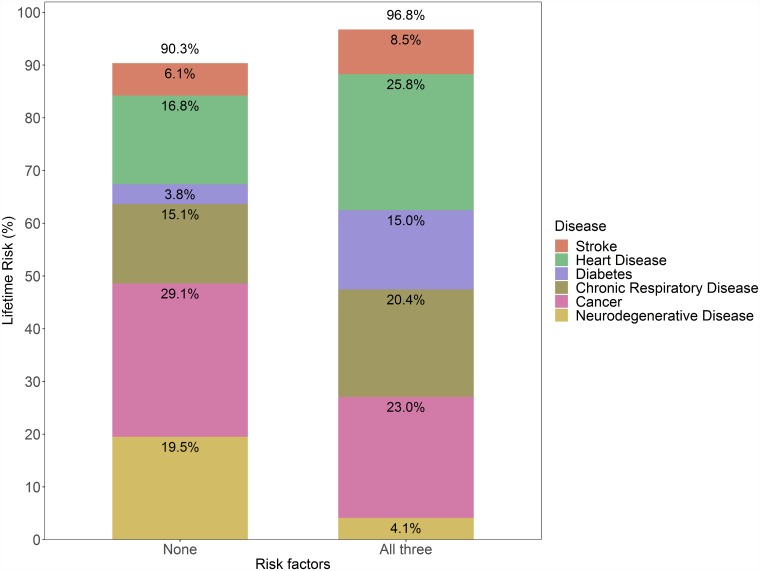
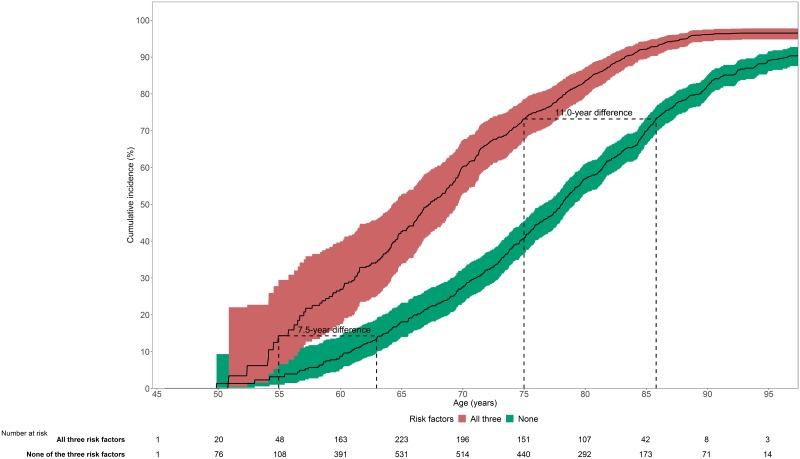
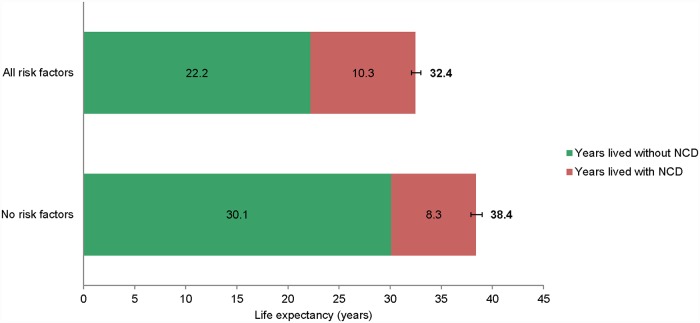
Methods and findings: Between July 6, 1989, and January 1, 2012, we followed participants from the prospective Rotterdam Study aged 45 years and older who were free from NCDs at baseline for incident stroke, heart disease, diabetes, chronic respiratory disease, cancer, and neurodegenerative disease. We quantified occurrence/co-occurrence and remaining lifetime risk of any NCD in a competing risk framework. We additionally studied the lifetime risk of any NCD, age at onset, and overall life expectancy for strata of 3 shared risk factors at baseline: smoking, hypertension, and overweight. During 75,354 person-years of follow-up from a total of 9,061 participants (mean age 63.9 years, 60.1% women), 814 participants were diagnosed with stroke, 1,571 with heart disease, 625 with diabetes, 1,004 with chronic respiratory disease, 1,538 with cancer, and 1,065 with neurodegenerative disease. NCDs tended to co-occur substantially, with 1,563 participants (33.7% of those who developed any NCD) diagnosed with multiple diseases during follow-up. The lifetime risk of any NCD from the age of 45 years onwards was 94.0% (95% CI 92.9%-95.1%) for men and 92.8% (95% CI 91.8%-93.8%) for women. These risks remained high (>90.0%) even for those without the 3 risk factors of smoking, hypertension, and overweight. Absence of smoking, hypertension, and overweight was associated with a 9.0-year delay (95% CI 6.3-11.6) in the age at onset of any NCD. Furthermore, the overall life expectancy for participants without these risk factors was 6.0 years (95% CI 5.2-6.8) longer than for those with all 3 risk factors. Participants aged 45 years and older without the 3 risk factors of smoking, hypertension, and overweight at baseline spent 21.6% of their remaining lifetime with 1 or more NCDs, compared to 31.8% of their remaining life for participants with all of these risk factors at baseline. This difference corresponds to a 2-year compression of morbidity of NCDs. Limitations of this study include potential residual confounding, unmeasured changes in risk factor profiles during follow-up, and potentially limited generalisability to different healthcare settings and populations not of European descent.
Conclusions: Our study suggests that in this western European community, 9 out of 10 individuals aged 45 years and older develop an NCD during their remaining lifetime. Among those individuals who develop an NCD, at least a third are subsequently diagnosed with multiple NCDs. Absence of 3 common shared risk factors is associated with compression of morbidity of NCDs. These findings underscore the importance of avoidance of these common shared risk factors to reduce the premature morbidity and mortality attributable to NCDs.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: LL has received unrestricted research awards/grants from AstraZeneca and Chiesi, and provided expert consultation for Boehringer Ingelheim GmbH and Novartis, outside of the submitted work. MJGL reports grants from Prins Bernhard Cultuurfonds 2014; grants from De Drie Lichten Foundation 2014; grants from Erasmus University Trustfonds 2014; personal fees from American Heart Association (AHA) 2014; personal fees from Netherlands Epidemiology Society (VvE) 2014; personal fees from European Society of Cardiology (ESC) 2013; personal fees from Dutch Heart Foundation (DHF) 2016; personal fees from Capri Cardiac Rehabilitation Foundation Rotterdam 2016; grants from Albert Schweitzer Hospital Research Fund 2018; grants from Oncology Research Albert Schweitzer (ORAS) Foundation 2018; grants from Promoting Advanced Cardiology through Education (PACE) Foundation 2018; all outside of the submitted work.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
