

Uneven terrain exacerbates the deficits of a passive prosthesis in the regulation of whole body angular momentum in individuals with a unilateral transtibial amputation
- PMID: 30717750
- PMCID: PMC6360756
- DOI: 10.1186/s12984-019-0497-9
Uneven terrain exacerbates the deficits of a passive prosthesis in the regulation of whole body angular momentum in individuals with a unilateral transtibial amputation
Abstract
Background: Uneven ground is a frequently encountered, yet little-studied challenge for individuals with amputation. The absence of control at the prosthetic ankle to facilitate correction for surface inconsistencies, and diminished sensory input from the extremity, add unpredictability to an already complex control problem, and leave limited means to produce appropriate corrective responses in a timely manner. Whole body angular momentum, L, and its variability across several strides may provide insight into the extent to which an individual can regulate their movement in such a context. The aim of this study was to explore L in individuals with a transtibial amputation, when challenged by an uneven surface. We hypothesized that, similar to previous studies, sagittal plane L would be asymmetrical on uneven terrain, and further, that uneven terrain would evoke a greater variability in L from stride to stride in individuals with amputation in comparison to unimpaired individuals, due to a limited ability to discern and correct for changing contours beneath the prosthetic foot.
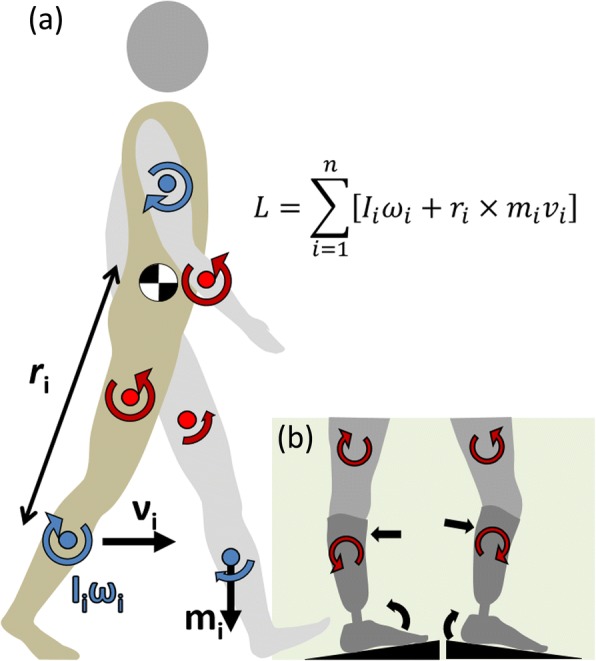
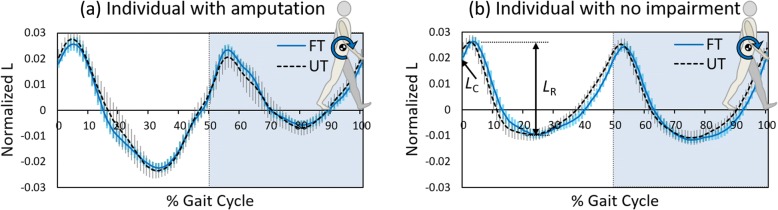
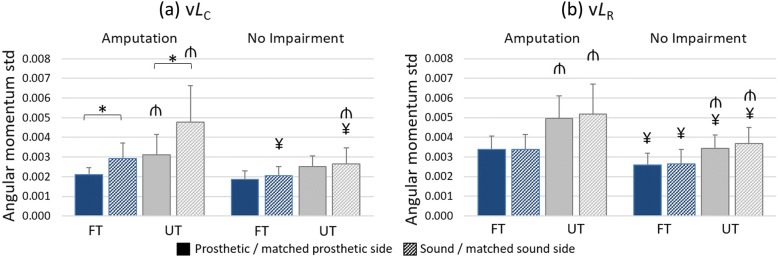
Methods: We examined sagittal plane L in ten individuals with a unilateral transtibial amputation and age- and gender- matched control participants walking on flat (FT) and uneven (UT) treadmills. The average range of L in the first 50% of the gait cycle (LR), the average L at foot contact (LC) and their standard deviations (vLR, vLC) were computed over 60 strides on each treadmill.
Results: On both surfaces we observed a higher LR on the prosthetic side and a reduced LC on the sound side (p < 0.001) in the amputee cohort, consistent with previous findings. UT invoked an increase in LC (p = 0.006), but not LR (p = 0.491). vLR, and vLC were higher in individuals with amputation (p < 0.001, p = 0.002), and increased in both groups on UT (p < 0.001).
Conclusions: These findings support previous assertions that individuals with amputation regulate L less effectively, and suggest that the deficits of the prosthesis are exacerbated on uneven terrain, potentially to the detriment of balance. Further, the results indicate that a greater demand may be placed on the unaffected side to control movement.
Keywords: Amputees; Angular momentum; Biomechanics; Gait; Motor learning; Passive prostheses; Uneven terrain.
Conflict of interest statement
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Patla AE, Shumway-Cook A. Dimensions of mobility: defining the complexity and difficulty associated with community mobility. J Aging Phys Act. 1999;7(1):7–19. doi: 10.1123/japa.7.1.7. - DOI
-
- Ülger Ö, Topuz S, Bayramlar K, Erbahçeci F, Sener G. Risk factors, frequency, and causes of falling in geriatric persons who has had a limb removed by amputation. Top Geriatr Rehabil. 2010;26(2):156–163. doi: 10.1097/TGR.0b013e3181e85533. - DOI
-
- Geurts AC, Mulder TW, Nienhuis B, Rijken RAJ. Postural reorganization following lower limb amputation. Possible motor and sensory determinants of recovery. Scand J Rehabil Med. 1992;24(2):83–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
